| Finasteride
5 vs finasteride 1 in androgenic alopecias./ Finasteride 5 vs finasteride
1 en alopecia androgenica
DATA-MEDICOS
DERMAGIC/EXPRESS 2-(95)
25 Septiembre 2.000 25 September 2.000
~Finasteride 5 vs finasteride 1 en alopecia androgenica ~
~ Finasteride 5 vs finasteride 1 in androgenic alopecia ~
EDITORIAL ESPANOL
=================
Hola amigos de la red DERMAGIC, de nuevo con ustedes con un tema bien
caliente:
FINASTERIDE 5 VS FINASTERIDE 1 EN ALOPECIA ANDROGENICA.
El primer trabajo que encontre sobre esta droga data del año
1.993 y otros mas de
1.994
donde se hablaba del FINASTERIDE COMO UNA DROGA promisoria en algunas
PATOLOGIAS COMO acne, hirsutismo, cancer de prostata e hiperplasia
prostatica,
PERO NUNCA se hablo del FINASTERIDE COMO una droga UTIL en la alopecia
androgenica hasta los años 1.998 cuando el laboratorio Merck
S. and Dhome decide
mercadear LA PROPECIA (finasteride 1 mgr) para su uso en la alopecia
androgenica.
Por supuesto ya se habia comprobado su efecto antiandrogenico.
Pero la pregunta es la siguiente ???. Porque el Laboratorio M.S.D
le quita 4 mgrs al
PROSCAR (finasteride 5 mgrs) para comercializarlo como un PRODUCTO
"NUEVO"
??? si ya para los años 1.995 se habia comprobado su eficacia
en la hiperplasia
prostatica. EXISTEN estudios donde a pacientes se les dio FINASTERIDE
5 MGRS
DIA POR 2 AÑOS SIN EFECTOS COLATERALES,
MAS AUN,, en el primer reporte de 1.993 se DEMOSTRO que dosis diarias
de 80
MGRS /dia de finasteride por 3 meses NO OCASIONABAN EFECTOS
SECUNDARIOS.
Por otra parte se ha demostrado que dosis diarias de PROPECIA (finasteride
1 mgr) han
provocado ginecomastia y adenomas, los cuales fueron reversibles con
la suspension del
tratamiento. Pero solo hay unos 3 0 4 casos reportados de una cohorte
de miles
pacientes
que ha tomado FINASTERIDE.
Desde que se conocio en el mundo cientifico QUE EL FINASTERIDE producia
crecimiento del cabello, comenzo a usarse el PROSCAR (FINASTERIDE 5
mgrs)
porque la PROPECIA (Finasteride 1 mgr) no habia salido al mercado.
La dosis: 10
MGRS SEMANALES en 2 dosis, martes y jueves con BUEN RESULTADO. Una
vez
salida la PROPECIA ( finasteride 1 mgr), el laboratorio comenzo una
AGRESIVA
CAMPAÑA descalificando este esquema terapeutico diciendo que
la dosis tenia que ser
un 1mgr dia por 7 dias a la semana. Pero la VERDAD es que FINASTERIDE
5 MGRS
2 VECES SEMANAL es tan bueno o superior al FINASTERIDE 1 MGR DIARIO,
y
el costo es muchisimo menor, mas seguro, menos riesgos. Una caja de
30 tab dura 15
semanas, (3 meses y 3 semanas). Entonces podriamos pensar LOGICAMENTE,
que el
laboratorio MERCK.S. DOHME lo que hizo fue mercadear un "viejo" y buen
producto,
reduciendo la dosis PARA QUE LO TOMARAMOS TODOS LOS DIAS, en fin una
mejor manera de "EXPLOTAR" la droga.
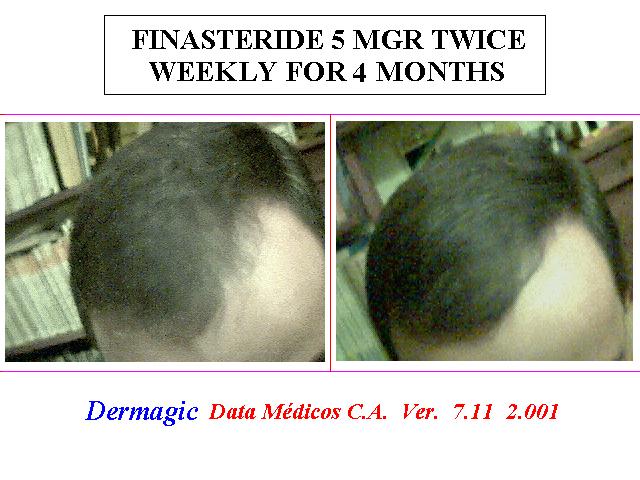
Yo me fui por el lado cientifico y comenze a probar el producto PROSCAR
(finasteride
5 mgrs) en pacientes con alopecia androgenica con el esquema antes
dicho 5 mgrs 2
veces semanal y al 4to mes observe mejoria notable de los pacientes,
vean las fotos del
attach.
He notado los siguientes efectos con el uso del FINASTERIDE:
Rapida repoblación del cabello areas frontal y occipital. MUCHO
MAS RAPIDA que
las fotos que nos muestra el LABORATORIO con 1 y 2 años de tratamiento
con
FINASTERIDE 1 MGR diario.
efectos adversos: NINGUNO, solo una leve disminucion de la cantidad
del volumen del
semen, de resto TODO NORMAL.. Otra cosa que he notado es una
RAPIDA
DESAPARICION DE CANAS, el cabello nuevo sale color marron !!!!.
En fin, puedo concluir que:
1.) EL FINASTERIDE ES UN producto maravilloso.
2.) FINASTRIDE 5 MGRS 2 veces semanal es MEJOR QUE FINASTERIDE 1 MGR
DIARIO.
3.) EL LABORATORIO MERCK.S.D LANZO la PROPECIA con fines
COMERCIALES Y DE MERCADEO.
4.) PROSTATA FELIZ, CABELLO NUEVO. !!!
No duden que por alli vendra el FINASTERIDE TOPICO, ya se esta hablando
de ello...
(referencia 33).
En estas 38 referencias, los hechos
Saludos a todos, hasta la proxima.
Dr. Jose Lapenta R.
EDITORIAL ENGLISH
=================
Hello friends of the net DERMAGIC, again with you with a very hot topic:
FINASTERIDE 5 VS FINASTERIDE 1 IN ANDROGENIC ALOPECIA
The first work that I found on this drug dates of the year 1.993 and
other but of 1.994
where it was spoken of the FINASTERIDE LIKE A promissory DRUG in some
PATHOLOGIES LIKE acne, hirsutism, prostate cancer and prostatic hyperplasia
, BUT
one NEVER speaks of the FINASTERIDE LIKE a USEFUL drug in the
ANDROGENIC ALOPECIA until the years 1.998 when the laboratory Merck
S. and
Dhome decides to market THE PROPECIA (finasteride 1 mgr) for its use
in the
androgenic alopecia. Of course already he had been proven their antiandrogenic
effect.
But is the question the following one???. Why the Laboratory
M.S.D remove him 4 mgrs
to the PROSCAR (finasteride 5 mgrs) to market it like a NEW PRODUCT???
if already
for the years 1.995 he had been proven their effectiveness in the prostatic
hyperplasia.
Studies EXIST where to patient they were given FINASTERIDE 5 MGRS DAY
FOR 2
YEARS WITHOUT COLATERAL EFFECTS, EVEN, in the first report of
1.993 it
was DEMONSTRATED that daily dose of 80 MGRS /day of finasteride for
3 months
didn't CAUSE SECONDARY EFFECTS.
On the other hand it has been demonstrated that daily dose of PROPECIA
(finasteride 1
mgr) they have caused gynecomastia and adenomas, which were reversible
with the
suspension of the treatment. But alone there are some 3 or 4 reported
cases of a cohort
thousand patients
that FINASTERIDE has taken.
Since it was known in the scientific world THAT THE FINASTERIDE produced
growth
of the hair, it began to be used the PROSCAR (FINASTERIDE 5 mgrs) because
the
PROPECIA (Finasteride 1 mgr) it had not left to the market. The dose:
10 WEEKLY
MGRS, Tuesday (5 MGRS) and Thursday (5 MGRS) with GOOD RESULT. Once
exit
the PROPECIA (finasteride 1 mgr), the laboratory began an AGGRESSIVE
CAMPAIGN disqualifying this therapeutic outline saying that the dose
had to be a 1mgr
day for 7 days a week.
But the TRUTH is that FINASTERIDE 5 MGRS TWICE WEEKLY it is so good
or
superior to the FINASTERIDE 1 MGRS DAILY and the cost is a lot
of minor, but sure,
less risks. A box of 30 tabs it is enough for 15 weeks, (3 months and
3 weeks). Then we
could think LOGICALLY that the laboratory MERCK.S. DOHME that made
it was TO
MARKET an "OLD" and good product, reducing the dose so that we TOOK
IT every
DAY, in short a better way of "EXPLODING"
the drug.
I left for the scientific side and began to prove the product PROSCAR
(finasteride 5
mgrs) in patient with androgenic alopecia and hirsutism with the outline
before said: 5
mgrs twice weekly and to the 4th month I observes the patients' remarkable
improvement, see the pictures in the attach.
I have noticed the following effects with the FINASTERIDE:
Quick repopulation of the hair areas frontal and occipital. A LOT BUT
QUICK that the
pictures that it shows us the LABORATORY with 1 and 2 years of treatment
with
FINASTERIDE 1 MGR daily. Adverse effects: NONE, alone a light decrease
of the
quantity of the volume of the semen, of rest ALL NORMAL one.. Another
thing that I
have noticed it is a QUICK DISAPPEARANCE OF GRAY-HEADED, the new hair
comes out brown color!!!!.
In short, I can conclude that:
1.) THE FINASTERIDE is A wonderful product.
2.) FINASTRIDE 5 MGRS twice weekly it is better than FINASTERIDE 1
MGR
DAILY.
3.) THE LABORATORY MERCK.S.D market the PROPECIA with COMMERCIAL
purpose AND OF MARKETING.
4.) HAPPY PROSTATE, NEW HAIR !!!
Don't doubt that over there the TOPICAL FINASTERIDE will come, already
some
people are speaking of it... (reference 33)
In these 38 references, the facts...
Until the next one
Greetings to all
Dr. Jose Lapenta R.,,,
==================================================================
REFERENCIAS BIBLIOGRAFICAS / BIBLIOGRAPHICAL REFERENCES
==================================================================
1.) Five-year follow-up of patients with benign prostatic hyperplasia
treated with
finasteride.
2.) Therapeutic effects of finasteride in benign prostatic hyperplasia:
a randomized
double-blind controlled trial.
3.) The effect of finasteride on prostate volume, urinary flow rate
and symptom score in
men with benign prostatic hyperplasia.
4.) [5-alpha-reductase inhibitors].
5.) Benign prostatic hyperplasia.
6.) The potential for hormonal prevention trials.
7.) 5 alpha-reductase inhibition by finasteride (Proscar) in epithelium
and stroma of human
benign prostatic hyperplasia.
8.) Pharmacological treatment of benign prostatic hyperplasia with
finasteride: a clinical
review.
9.) Medical therapy for benign prostatic hyperplasia: A review of the
literature.
10.) Pretreatment with finasteride decreases perioperative bleeding
associated with
transurethral resection of the prostate.
11.) Urinary retention in patients with BPH treated with finasteride
or placebo over 4
years. Characterization of patients and ultimate outcomes.The PLESS
Study Group.
12.) Dihydrotestosterone and the concept of 5alpha-reductase inhibition
in human benign
prostatic hyperplasia.
13.) Chronic treatment with finasteride daily does not affect spermatogenesis
or semen
production in young men.
14.) Management of androgenetic alopecia.
15.) Finasteride in the treatment of men with frontal male pattern
hair loss.
16.) Androgenetic alopecia in men: the scale of the problem and prospects
for treatment.
17.) [Androgenetic alopecia, hirsutism and hypertrichosis].
18.) Medical treatments for balding in men.
19.) Understanding and managing common baldness.
20.) Finasteride: a review of its use in male pattern hair loss.
21.) Finasteride in the treatment of men with androgenetic alopecia.
Finasteride Male
Pattern Hair Loss Study Group.
22.) Genetic analysis of male pattern baldness and the 5alpha-reductase
genes.
23.) Effect of finasteride on human testicular steroidogenesis.
24.) [Finasteride: a new drug for the treatment of male hirsutism and
androgenetic
alopecia]?
25.) The 5 alpha-reductase system and its inhibitors. Recent development
and its
perspective in treating androgen-dependent skin disorders.
26.) Finasteride: a clinical review.
27.) The effect of finasteride, a 5 alpha-reductase inhibitor, on scalp
skin testosterone and
dihydrotestosterone concentrations in patients with male pattern baldness.
28.) Finasteride: the first 5 alpha-reductase inhibitor.
29.) Cytologic atypia in a 53-year-old man with finasteride-induced
gynecomastia.
30.) Reversible painful gynaecomastia induced by low dose finasteride
(1 mg/day).
31.) Measuring reversal of hair miniaturization in androgenetic alopecia
by follicular counts
in horizontal sections of serial scalp biopsies: results of finasteride
1 mg treatment of men
and postmenopausal women.
32.) Improvement in androgenetic alopecia in 53-76-year-old men using
oral finasteride.
33.) New topical antiandrogenic formulations can stimulate hair growth
in human bald
scalp grafted onto mice.
34.) Current management of androgenetic alopecia in men.
35.) Immunohistochemical localization of types 1 and 2 5alpha-reductase
in human scalp.
36.) The psychosocial consequences of androgenetic alopecia: a review
of the research
literature.
37.) Clinical dose ranging studies with finasteride, a type 2 5alpha-reductase
inhibitor, in
men with male pattern hair loss.
38.) The effects of finasteride on scalp skin and serum androgen levels
in men with
androgenetic alopecia.
=============================================================
=============================================================
1.) Five-year follow-up of patients with benign prostatic hyperplasia
treated with
finasteride.
=============================================================
Eur Urol 1995;27(4):267-73
Geller J
Mercy Hospital and Medical Center, San Diego, CA 92103-2180, USA.
In 18 of 55 original patients who completed 5 years of treatment with
finasteride,
significant reductions in prostate size were noted at 1 year and sustained
thereafter.
Symptom scores in these same patients were significantly improved or
stable over the 5
years while maximal urinary flow rates were unchanged. Data from 15
of 18 other
patients who dropped out of the study before 5 years showed changes
in prostate size,
symptom score and flow rates that were similar to those noted in patients
treated for 5
years. No side effects were noted in this study except for sexual dysfunction,
which
occurred in less than 5% of the patients. With few exceptions, finasteride
appears to
arrest the process of BPH over a 5 year period as indicated by sustained
reductions in
prostate size accompanied by either symptomatic improvement or stability
in all other
patients.
=============================================================
2.) Therapeutic effects of finasteride in benign prostatic hyperplasia:
a randomized
double-blind controlled trial.
=============================================================
J Formos Med Assoc 1995 Jan-Feb;94(1-2):37-41
Yu HJ, Chiu TY, Lai MK
Department of Urology, National Taiwan University Hospital, Taipei,
R.O.C.
The clinical effects of finasteride, a 5 alpha-reductase inhibitor,
in patients with benign
prostatic hyperplasia (BPH) were evaluated in a double-blind, placebo-controlled
study.
Forty-six patients with symptomatic BPH were randomly assigned to 2
groups, the
finasteride group and the placebo group. The finasteride group received
5 mg of
finasteride daily for 6 months. Prostate volume, urinary flow, urinary
symptoms, serum
prostate-specific antigen (PSA) and adverse events were determined
before and after
treatment. After 6 months of treatment the patients treated with 5
mg of finasteride per
day had a 30% decrease in their total urinary symptom score, a 14%
decrease in prostate
volume and a 0.9 ng/dL decrease of PSA. Their maximal urinary flow
rate increased by
1.42 mL per second and the mean urinary flow rate increased by 0.64
mL per second.
The patients given placebo showed no significant changes in their prostate
volume, serum
PSA and maximal and mean urinary flow rate. However, the symptom scores
in the
placebo group also decreased significantly. When compared with the
placebo group,
those in the finasteride group had significantly lower prostate volume,
serum PSA,
maximal urinary flow rate and urinary symptoms, but not mean urinary
flow rate. The
frequency of adverse events was low in both the finasteride and placebo
groups. These
results show that finasteride may be an effective and safe alternative
for the treatment of
patients with BPH.
=============================================================
3.) The effect of finasteride on prostate volume, urinary flow rate
and symptom score in
men with benign prostatic hyperplasia.
=============================================================
Aust N Z J Surg 1995 Jan;65(1):35-9
Nacey JN, Meffan PJ, Delahunt B
Department of Surgery, Wellington School of Medicine, New Zealand.
This study was designed to determine the efficacy of the 5 alpha-reductase
inhibitor
finasteride (Proscar, MK-906) in men with reduced urinary flow rates
and symptoms of
urinary outflow obstruction secondary to benign prostatic hyperplasia.
Forty-five men
were randomized to one of three groups receiving either placebo, 1
mg/day or 5 mg/day
finasteride for the first 12 months of the study period. At the end
of this period all men
received 5 mg/day finasteride for a further 2 years. Efficacy was determined
by
measurement of prostate volume, maximum urinary flow rate, and symptom
score using a
modified Boyarsky assessment. Prostate volume reduced by 20 and 27%,
respectively,
for those on 1 and 5 mg after the first year. At 3 years the volume
had reduced by 43%.
This reduction in prostate volume was associated with an improvement
in maximum
urinary flow rate by 50% (1 mg), and 35% (5 mg) at 1 year, and 36%
at 3 years. The
total, obstructive and non-obstructive symptom scores decreased (improved)
for patients
on 1 and 5 mg finasteride, with the total score reducing by 33% from
baseline at year 3.
The results demonstrate that finasteride causes a modest but significant
clinical
improvement in men with urinary outflow obstruction secondary to benign
prostatic
hyperplasia.
=============================================================
4.) [5-alpha-reductase inhibitors].
=============================================================
Acta Urol Belg 1994 Dec;62(4):23-31
De Jaegher K, Kozyreff P, Claes H
A reflection is made, on the one hand, on the lack of correlation between
the intensity of
micturition problems and the volume of the prostate and, on the other
hand, on the
different therapeutic approaches of irritative or obstructive voiding
problems, and finally
on the insufficiently convincing activity of Finasteride.
=============================================================
5.) Benign prostatic hyperplasia.
=============================================================
Endocrinol Metab Clin North Am 1994 Dec;23(4):795-807
Jonler M, Riehmann M, Brinkmann R, Bruskewitz RC
Division of Urology, University of Wisconsin, Madison.
Benign prostatic hyperplasia (BPH) is the most common cause of bladder
outlet
obstruction and voiding symptoms in elderly men. The pathogenesis is
not fully determined
but a combination of androgens and age are needed for development of
BPH. Symptoms
of BPH are divided into obstructive and irritative symptoms but large
interpersonal
variability is found and no specific BPH symptom exists. Treatment
modalities include
surgery (TURP, TUIP, open prostatectomy, laser ablation, balloon dilatation,
hyperthermia and thermotherapy, and urethral stents) and medical therapy.
TURP is the
gold standard treatment and TUIP is a safe and effective alternative
to TURP in patients
with smaller prostates. Laser ablation, hyperthermia and thermotherapy,
and urethral
stents are at the present time under investigation. Balloon dilatation
is FDA-approved but
not often used because of low efficacy and poor long-term results.
Medical treatment
includes alpha-blocker or finasteride treatment and is indicated in
patients with moderate
to severe symptoms of BPH without a strong indication for surgery.
=============================================================
6.) The potential for hormonal prevention trials.
=============================================================
Cancer 1994 Nov 1;74(9 Suppl):2726-33
Ford LG, Brawley OW, Perlman JA, Nayfield SG, Johnson KA, Kramer BS
Detection and Community Oncology Program, National Cancer Institute,
Bethesda,
Maryland 20892.
Breast and prostate cancer are significant causes of morbidity and mortality
and are very
similar in etiology, epidemiology, and modalities of treatment. Investigational
strategies in
the prevention of these malignancies also have strong parallels. The
National Cancer
Institute is sponsoring several large scale clinical trials involving
hormonal manipulation and
cancer prevention. In the Breast Cancer Prevention Trial, 16,000 women
at high risk for
breast cancer are being randomized to receive the antiestrogen agent
tamoxifen or
placebo for 5 years in an effort to determine if breast cancer development
can be
inhibited. In a similar trial, the Prostate Cancer Prevention Trial,
18,000 men older than
55 years of age will be randomized to receive finasteride, a 5-alpha-reductase
inhibitor,
or placebo to determine if inhibition of dihydrotestosterone synthesis
in the prostate over a
prolonged period will lead to a decreased incidence of prostate cancer.
Both clinical trials
offer the possibility of demonstrating that a hormonal intervention
can decrease an
individual's risk of developing breast or prostate cancer. They also
have the potential of
providing critical information about cancer risk, etiology, screening,
and genetics, as well
as quantifying the risks and benefits of specific preventive interventions.
=============================================================
7.) 5 alpha-reductase inhibition by finasteride (Proscar) in epithelium
and stroma of human
benign prostatic hyperplasia.
=============================================================
Steroids 1994 Nov;59(11):616-20
Weisser H, Tunn S, Debus M, Krieg M
Institute of Clinical Chemistry and Laboratory Medicine, University
Clinic Bergmannsheil,
Bochum, Germany.
Finasteride is a specific 5 alpha-reductase inhibitor that has been
shown to reduce the size
of human benign prostatic hyperplasia (BPH) by inhibiting the intraprostatic
conversion of
testosterone to 5 alpha-dihydrotestosterone. The aim of the present
in vitro study was to
describe in more detail the inhibitory effect of finasteride on 5 alpha-reductase
in
epithelium and stroma of human BPH. 5 alpha-Reductase activity in epithelium
and
stroma was inhibited dose-dependently by finasteride. The mean IC50
(50% inhibitory
concentration) values, determined in the presence of various testosterone
concentrations,
were generally 2- to 4-fold lower in epithelium than in stroma. With
finasteride
concentrations greater than 5 nM, competitive inhibition of 5 alpha-reductase
occurred
both in epithelium and stroma. The mean inhibition constant Ki[nM +/-
SEM] was 7 +/- 3
and 31 +/- 3 in epithelium and stroma, respectively. In the presence
of finasteride
concentrations < or = 5 nM, the epithelial 5 alpha-reductase seems
to be inhibited in an
uncompetitive manner, whereas such low finasteride concentrations cause
either no
inhibition (1-2 nM) or competitive inhibition (5 nM) in stroma. Our
present study provides
evidence that the inhibitory effect of finasteride on 5 alpha-reductase
is much stronger in
epithelium than in stroma. Therefore, it is conceivable that the global
size-reduction of
BPH under finasteride treatment is primarily due to the regression
of BPH epithelium.
=============================================================
8.) Pharmacological treatment of benign prostatic hyperplasia with
finasteride: a clinical
review.
=============================================================
Arch Esp Urol 1994 Nov;47(9):883-7; discussion 887-8
Ekman P
Department of Urology, Karolinska Hospital, Stockholm, Sweden.
Finasteride acts by blocking the conversion of testosterone to 5
alpha-dihydrotestosterone, the active androgen metabolite in the human
prostate. In large,
double-blind, placebo-controlled phase III studies recruiting over
1600 patients, it was
shown that the administration of Finasteride, either 5 or 1 mg a day,
reduced the size of
the prostate by a mean of 22%, following 6 months of therapy. Despite
this reduction in
prostate size, urinary flow rate only improved by a mean of 1.7 ml
per second and
symptom score improved only marginally, but statistically significantly
different from
placebo. Long-term results in small series of patients have indicated
a further
improvement beyond 1 year. After 3 years flow was improved by 60%.
The future role
for Finasteride therapy is emerging, but it appears as if patients
with mild to moderate
symptoms would be a group who could benefit the most. Whether or not
Finasteride can
stop the long-term natural course of benign prostatic hyperplasia has
still to be
demonstrated.
=============================================================
9.) Medical therapy for benign prostatic hyperplasia: A review of the
literature.
=============================================================
Eur Urol 2000 Jul;38(1):2-19
Clifford GM, Farmer RD
Public Health and Primary Care Research Unit, European Institute of
Health and Medical
Sciences, University of Surrey, Surrey Research Park, UK.
[Medline record in process]
OBJECTIVE: To review the existing evidence regarding the efficacy and
safety of
medical therapy for lower urinary tract symptoms (LUTS) indicative
of benign prostatic
hyperplasia (BPH). To assess randomised controlled trials investigating
the six
alpha-adrenergic receptor antagonists (alpha-blockers), prazosin, alfuzosin,
indoramin,
terazosin, doxazosin, and tamsulosin, that benefit patients by relaxing
prostatic smooth
muscle, and the anti-androgen, finasteride, that mediates its more
long-term benefits by
reducing prostate size. RESULTS: This review suggests that both classes
of drug offer
significant improvement in criteria used to evaluate symptomatic BPH
and can be effective
whilst being acceptably safe. Furthermore, the therapeutic efficacy
of all contemporary
alpha-blockers appear similar, both in terms of symptom relief and
urodynamic
improvements. Randomised controlled trials have additionally demonstrated
that
finasteride therapy can provide improvement in terms of quality of
life indices, prostate
volume, and risks of progressing to acute urinary retention or prostatic
surgery. While
alpha-blockers have a rapid onset of action, likely to produce a therapeutic
result within
weeks, regardless of whether prostatic enlargement or bladder outlet
obstruction is
present, finasteride appears to be effective for more long-term therapy
for up to 4 years,
but only in alleviating symptoms when they are associated with a significantly
large
prostate. Neither finasteride nor the alpha(1a)-receptor-selective
blocker, tamsulosin, are
associated with the lowering of blood pressure and incidence of cardiovascular
side
effects that are apparent with other less selective alpha-blocker therapies
such as
dizziness and postural hypertension. They are, however, both associated
with an
increased risk of sexual dysfunction, albeit less than those associated
with surgical
intervention. Whereas tamsulosin is associated only with ejaculatory
dysfunction,
finasteride is additionally linked to decreased libido and impotence.
=============================================================
10.) Pretreatment with finasteride decreases perioperative bleeding
associated with
transurethral resection of the prostate.
=============================================================
Urology 2000 May;55(5):684-9
Hagerty JA, Ginsberg PC, Harmon JD, Harkaway RC
Department of Surgery, Division of Urology, Albert Einstein Medical
Center and
Philadelphia College of Osteopathic Medicine, Philadelphia, Pennsylvania,
USA.
OBJECTIVES: The efficacy of finasteride in the treatment of gross hematuria
associated
with benign prostatic hyperplasia is well established. We evaluated
a regimen of
pretreatment with finasteride in decreasing perioperative bleeding
associated with
transurethral resection of the prostate (TURP). METHODS: A prospective
analysis
compared 25 patients pretreated with finasteride for 2 to 4 months
before TURP with 50
patients without pretreatment. Patients in each group were further
separated by the
amount of prostate tissue resected. Patients were then followed up
for perioperative
bleeding, defined as a perioperative blood transfusion requirement
or a return visit to the
emergency room with gross hematuria or clot retention. RESULTS: None
of the patients
with less than 30 g of prostate tissue resected experienced perioperative
bleeding. In
patients with 30 g or more resected, several episodes of bleeding occurred.
In the
patients pretreated with finasteride, 1 (8.3%) of 12 experienced perioperative
bleeding; in
the control group, 7 (36.8%) of 19 had an episode of bleeding. CONCLUSIONS:
In
patients with large prostate glands undergoing TURP, pretreatment with
finasteride
appears useful in reducing perioperative bleeding.
=============================================================
11.) Urinary retention in patients with BPH treated with finasteride
or placebo over 4
years. Characterization of patients and ultimate outcomes.The PLESS
Study Group.
=============================================================
Eur Urol 2000 May;37(5):528-36
Roehrborn CG, Bruskewitz R, Nickel GC, Glickman S, Cox C, Anderson R,
Kandzari
S, Herlihy R, Kornitzer G, Brown BT, Holtgrewe HL, Taylor A, Wang D,
Waldstreicher
J
The University of Texas Southwestern Medical Center, Dallas, TX 07525-9110,
USA.
[email protected]
OBJECTIVES: Knowledge regarding the incidence and prevalence of acute
urinary
retention and the ultimate outcome is very limited. The purpose of
the present analysis
was to document the natural history and outcomes of acute urinary retention
(AUR)
further specified as being either precipitated or spontaneous, and
to evaluate the potential
benefit of finasteride therapy. MATERIALS AND METHODS: Three thousand
and
forty men with moderate to severe symptoms of BPH and enlarged prostate
glands by
digital rectal examination were enrolled into the 4-year placebo-controlled
PLESS trial
and were evaluated for occurrences of AUR and BPH-related surgery.
Men in the study
were seen every 4 months; discontinued patients were followed up 6
months after
discontinuation and again at the end of the 4-year trial. Complete
4-year data on
outcomes (occurrence of AUR or BPH-related surgery) was available for
92% of the
enrolled subjects in each treatment group. An endpoint committee, blinded
to treatment
group and center, reviewed and categorized all study-related documentation
relating to
retention and surgery. RESULTS: Over the 4-year period, 99 of 1,503
placebo-treated
patients (6.6%) experienced one or more episodes of AUR in comparison
with 42 or
1,513 finasteride-treated patients (2.8%; p<0. 001). Approximately
half of the episodes
of retention were spontaneous and clearly BPH-related, while the other
episodes were
precipitated by another factor (PAUR). After spontaneous AUR, subsequent
surgery was
performed in 39 of 52 (75%) placebo-treated patients versus 8 of 20
(40%)
finasteride-treated patients (p = 0. 01). BPH-related surgery was less
common in men
who had a prior episode of PAUR (26% in the placebo group and 14% in
the finasteride
group). CONCLUSION: There is a continual risk of spontaneous and precipitated
acute
urinary retention in men with moderate to severe lower urinary tract
symptoms and an
enlarged prostate gland. Fewer patients who developed precipitated
AUR than
spontaneous AUR go on to need subsequent BPH-related surgery. Significantly
fewer
finasteride-than placebo-treated patients developed AUR, and among
those men, fewer
ultimately needed BPH-related surgery.
=============================================================
12.) Dihydrotestosterone and the concept of 5alpha-reductase inhibition
in human benign
prostatic hyperplasia.
=============================================================
Eur Urol 2000 Apr;37(4):367-80
Bartsch G, Rittmaster RS, Klocker H
Department of Urology, University of Innsbruck, Austria. [email protected]
OBJECTIVE:The development of the human benign prostatic hyperplasia
clearly requires
a combination of testicular androgens and aging. Although the role
of androgens as the
causative factor for human benign prostatic hyperplasia is debated,
they undoubtedly have
at least a permissive role. The principal prostatic androgen is dihydrotestosterone
(DHT).
Although not elevated in human benign prostatic hyperplasia, DHT levels
in the prostate
remain at a normal level with aging, despite a decrease in the plasma
testosterone.
RESULTS: DHT is generated by reduction of testosterone. Two isoenzymes
of
5alpha-reductase have been discovered. Type 1 is present in most tissues
of the body
where 5alpha-reductase is expressed and is the dominant form in sebaceous
glands.
Type2 5alpha-reductase is the dominant isoenzyme in genital tissues,
including the
prostate. Finasteride is a 5alpha-reductase inhibitor that has been
used for the treatment
of benign prostatic hyperplasia and male-pattern baldness. At doses
used clinically, its
major effect is through suppression of type 2 5alpha-reductase, because
it has a much
lower affinity for the type 1 isoenzyme. Finasteride suppresses DHT
by about 70% in
serum and by as much as 85-90% in the prostate. The remaining DHT in
the prostate is
likely to be the result of type 1 5alpha-reductase. Suppression of
both 5alpha-reductase
isoenzymes with GI198745 result in greater and more consistent suppression
of serum
dihydrotestosterone than that observed with a selective inhibitor of
type 2
5alpha-reductase. Physiological and clinical studies comparing dual
5alpha-reductase
inhibitors, such as GI198745, with selective type 2, such as finasteride,
will be needed to
determine the clinical relevance of type 1 5alpha-reductase within
the prostate. Two large
international multicenter, phase III trials have been published documenting
the safety and
efficacy of finasteride in the treatment of human benign prostatic
hyperplasia. Combining
these two studies, randomized, controlled data are available for 12
months.
Noncontrolled extension of these data from a subset of patients, who
elected to continue
drug treatment for 3, 4 or 5 years, are also available. Long-term medical
therapy with
finasteride can reduce clinically significant endpoints such as acute
urinary retention or
surgery. According to the meta-analysis of six randomised clinical
trial with finasteride,
finasteride is most effective in men with large prostates. A more effective
dual inhibitor of
type 1 and 2 human 5alpha-reductase may lower circulating DHT to a
greater extent than
finasteride and show advantages in the treatment of human benign prostatic
hyperplasia
and other disease states that depend on DHT. CONCLUSION: Clinical evaluation
of
potent dual 5alpha-reductase inhibitors may help define the relative
roles of human type 1
and 2 5alpha-reductase in the pathophysiology of benign prostatic hyperplasia
and other
androgen-dependent diseases.
=============================================================
13.) Chronic treatment with finasteride daily does not affect spermatogenesis
or semen
production in young men.
=============================================================
J Urol 1999 Oct;162(4):1295-300 Related Articles, Books, LinkOut
Overstreet JW, Fuh VL, Gould J, Howards SS, Lieber MM, Hellstrom W,
Shapiro S,
Carroll P, Corfman RS, Petrou S, Lewis R, Toth P, Shown T, Roy J, Jarow
JP, Bonilla
J, Jacobsen CA, Wang DZ, Kaufman KD
Department of Obstetrics and Gynecology, University of California, Davis,
USA.
PURPOSE: Finasteride, an oral type 2, 5alpha-reductase inhibitor, is
used in 1 mg. daily
doses for the treatment of male pattern hair loss. A dose of 5 mg.
finasteride daily reduces
ejaculate volume by approximately 25%, and reduces prostate volume
by approximately
20% and serum prostate specific antigen (PSA) by approximately 50%
in men with
benign prostatic hyperplasia. To our knowledge no data exist on the
effect of 1 mg.
finasteride daily on ejaculate volume or other semen parameters, or
on the prostate in
young men. Therefore, we studied the potential effect and reversibility
of effect of 1 mg.
finasteride daily on spermatogenesis, semen production, the prostate
and serum PSA in
young men. MATERIALS AND METHODS: In this double-blind, placebo controlled
multicenter study 181 men 19 to 41 years old were randomized to receive
1 mg.
finasteride or placebo for 48 weeks followed by a 60-week off-drug
period. Of the 181
men 79 were included in a subset for the collection and analysis of
sequential semen
samples. RESULTS: There were no significant effects of 1 mg. finasteride
on sperm
concentration, total sperm per ejaculate, sperm motility or morphology.
Ejaculate volume
in subjects on finasteride decreased 0.3 ml. (-11%) compared to a decrease
of 0.2 ml.
(-8%) for placebo, with a median between treatment group difference
of -0.03 ml. (1%,
90% confidence interval -10.4 to 13.1, p = 0.915). There were significant
but small
decreases in prostate volume (-2.6%) and serum PSA (-0.2 ng./ml.) in
the finasteride
group, which reversed on discontinuation of the drug. CONCLUSIONS:
Treatment with
1 mg. finasteride daily for 48 weeks did not affect spermatogenesis
or semen production
in young men. The effects of 1 mg. finasteride daily on prostate volume
and serum PSA in
young men without benign prostatic hyperplasia were small and reversible
on
discontinuation of the drug.
=============================================================
14.) Management of androgenetic alopecia.
=============================================================
J Eur Acad Dermatol Venereol 1999 May;12(3):205-14 Related Articles,
Books,
LinkOut
Tosti A, Camacho-Martinez F, Dawber R
Department of Dermatology, University of Bologna, Italy. [email protected]
BACKGROUND: Androgenetic alopecia (AGA) is the most frequent cause of
hair loss
affecting up to 50% of men and 40% of women by the age of 50. METHODS:
This
paper outlines the current status of diagnosis and offers guidelines
for optimal management
of AGA in both men and women. RESULTS: The diagnosis of AGA can usually
be
confirmed by medical history and physical examination alone. A trichogram
can be useful
to assess the progression of the hair loss. A scalp biospy is diagnostic
but usually not
required. In women with signs of hyperandrogenism, investigation for
ovarian (polycystic
ovarian disease) or adrenal (late-onset congenital adrenal hyperplasia)
disorders is
required. Mild to moderate AGA in men can be treated with oral finasteride
or topical
minoxidil. Oral finasteride at the dosage of 1 mg/day produced clinical
improvement in up
to 66% of patients treated for 2 years. The drug is effective for both
frontal and vertex
hair thinning. Medical treatment with finasteride or minoxidil should
be continued
indefinitely since interruption of therapy leads to hair loss with
return to pretreatment
status. Mild to moderate AGA in women can be treated with oral antiandrogens
(cyproterone acetate, spironolactone) and/or topical minoxidil with
good results in many
cases. Hair systems and surgery may be considered for selected cases
of severe AGA
both in men and in women. CONCLUSIONS: Patients with AGA should be
informed
about the pathogenesis of the condition. If used correctly, available
medical treatments
arrest progression of the disease and reverse miniaturization in most
patients with mild to
moderate AGA.
=============================================================
15.) Finasteride in the treatment of men with frontal male pattern
hair loss.
=============================================================
J Am Acad Dermatol 1999 Jun;40(6 Pt 1):930-7 Related Articles, Books,
LinkOut
Leyden J, Dunlap F, Miller B, Winters P, Lebwohl M, Hecker D, Kraus
S, Baldwin H,
Shalita A, Draelos Z, Markou M, Thiboutot D, Rapaport M, Kang S, Kelly
T, Pariser D,
Webster G, Hordinsky M, Rietschel R, Katz HI, Terranella L, Best S,
Round E,
Waldstreicher J
University of Pennsylvania School of Medicine, Philadelphia, USA.
BACKGROUND: Finasteride, a specific inhibitor of type II 5alpha-reductase,
decreases
serum and scalp dihydrotestosterone and has been shown to be effective
in men with
vertex male pattern hair loss. OBJECTIVE: This study evaluated the
efficacy of
finasteride 1 mg/day in men with frontal (anterior/mid) scalp hair
thinning. METHODS:
This was a 1-year, double-blind, placebo-controlled study followed
by a 1-year open
extension. Efficacy was assessed by hair counts (1 cm2 circular area),
patient and
investigator assessments, and global photographic review. RESULTS:
There was a
significant increase in hair count in the frontal scalp of finasteride-treated
patients (P <
.001), as well as significant improvements in patient, investigator,
and global photographic
assessments. Efficacy was maintained or improved throughout the second
year of the
study. Finasteride was generally well tolerated. CONCLUSION: In men
with hair loss in
the anterior/mid area of the scalp, finasteride 1 mg/day slowed hair
loss and increased hair
growth.
=============================================================
16.) Androgenetic alopecia in men: the scale of the problem and prospects
for treatment.
=============================================================
Int J Clin Pract 1999 Jan-Feb;53(1):50-3 Related Articles, Books, LinkOut
Rushton DH
School of Pharmacy and Biomedical Sciences, University of Portsmouth,
Hants.
While the precise incidence of androgenetic alopecia is unknown, it
is universally
acknowledged to be the most common hair problem in men. Balding is
generally
associated with ageing; consequently, the desire to prolong a youthful
appearance
inevitably leads to demands for effective treatments. Further, changing
attitudes in modern
society have resulted in people becoming concerned about their appearance
and less
tolerant about conditions that might be alleviated by medical intervention.
The importance
of hair loss upon quality of life has been underestimated by the medical
profession.
Clinicians failing to accept hair loss as an important medical problem
ignore the real
distress suffered by a significant proportion of those affected. New
options for treatment
that selectively target the metabolic pathways involved in the balding
process are showing
promise. The first generation of such drugs, Propecia, is now available
in some countries
and other molecules are currently under development.
=============================================================
17.) [Androgenetic alopecia, hirsutism and hypertrichosis].
=============================================================
Ther Umsch 1999 Apr;56(4):219-24 Related Articles, Books, LinkOut
Trueb RM, Wyss M, Itin PH
Dermatologische Klinik, Universitatsspital Zurich.
Having too much hair on the face or the body and not enough on the scalp
respectively, is
generally not a mirror of a life-threatening disease. However, the
emotional impact of such
cosmetic problems may be remarkable in the individual case. Currently
rational treatment
options are becoming increasingly available to correct such hair problems.
This review
highlights the new therapeutic achievements in the treatment of both
androgenetic alopecia
and hirsutism. Oral treatment of male patterned hair loss with finasteride
in men is
emphasized, and the use of antiandrogens in women is discussed. In
addition, the mode of
action and clinical results of topical minoxidil treatment find mention.
The second part of
the review deals with hirsutism and hypertrichosis. The diagnostic
steps and investigations
are briefly reviewed, and the advances in laser treatment of hirsutism
and hypertrichosis
are presented.
=============================================================
18.) Medical treatments for balding in men.
=============================================================
Am Fam Physician 1999 Apr 15;59(8):2189-94, 2196 Related Articles,
Books,
LinkOut
Scow DT, Nolte RS, Shaughnessy AF
Harrisburg Family Practice Residency, PA 17105-8700, USA.
Two drugs are available for the treatment of balding in men. Minoxidil,
a topical product,
is available without a prescription in two strengths. Finasteride is
a prescription drug taken
orally once daily. Both agents are modestly effective in maintaining
(and sometimes
regrowing) hair that is lost as a result of androgenic alopecia. The
vertex of the scalp is the
area that is most likely to respond to treatment, with little or no
hair regrowth occurring on
the anterior scalp or at the hairline. Side effects of these medications
are minimal, making
them suitable treatments for this benign but psychologically disruptive
condition.
=============================================================
19.) Understanding and managing common baldness.
=============================================================
Aust Fam Physician 1999 Mar;28(3):248-50, 252-3
Tran D, Sinclair RD
Department of Dermatology, St Vincent's Hospital, Melbourne.
BACKGROUND: Society places importance on physical attributes especially
the
appearance of our hair. Common baldness or androgenetic alopecia is
a normal
physiological process of hair loss in genetically predisposed individuals.
Premature or
accelerated hair loss can engender considerable negative thoughts and
anxiety associated
with feelings of diminished attractiveness. OBJECTIVE: To enable general
practitioners to
recognise the various treatment options available, therefore offering
patients reasonable
hope and informed choices. DISCUSSION: Common baldness can be prevented
by
currently available mediums and regrowth may be achieved in a significant
percentage of
cases. Correct use of these agents requires an understanding of the
pathogenesis of
androgenetic alopecia, its natural history and the time course of response
to treatment.
=============================================================
20.) Finasteride: a review of its use in male pattern hair loss.
=============================================================
Drugs 1999 Jan;57(1):111-26 Related Articles, Books, LinkOut
McClellan KJ, Markham A
Adis International Limited, Mairangi Bay, Auckland, New Zealand. [email protected]
The 5alpha-reductase inhibitor finasteride blocks the conversion of
testosterone to
dihydrotestosterone (DHT), the androgen responsible for male pattern
hair loss
(androgenetic alopecia) in genetically predisposed men. Results of
phase III clinical
studies in 1879 men have shown that oral finasteride 1 mg/day promotes
hair growth and
prevents further hair loss in a significant proportion of men with
male pattern hair loss.
Evidence suggests that the improvement in hair count reported after
1 year is maintained
during 2 years' treatment. In men with vertex hair loss, global photographs
showed
improvement in hair growth in 48% of finasteride recipients at 1 year
and in 66% at 2
years compared with 7% of placebo recipients at each time point. Furthermore,
hair
counts in these men showed that 83% of finasteride versus 28% of placebo
recipients had
no further hair loss compared with baseline after 2 years. The clinical
efficacy of oral
finasteride has not yet been compared with that of topical minoxidil,
the only other drug
used clinically in patients with male pattern hair loss. Therapeutic
dosages of finasteride
are generally well tolerated. In phase III studies, 7.7% of patients
receiving finasteride 1
mg/day compared with 7.0% of those receiving placebo reported treatment-related
adverse events. The overall incidence of sexual function disorders,
comprising decreased
libido, ejaculation disorder and erectile dysfunction, was significantly
greater in finasteride
than placebo recipients (3.8 vs 2.1%). All sexual adverse events were
reversed on
discontinuation of therapy and many resolved in patients who continued
therapy. No other
drug-related events were reported with an incidence > or =1% in patients
receiving
finasteride. Most events were of mild to moderate severity. Oral finasteride
is
contraindicated in pregnant women because of the risk of hypospadias
in male fetuses.
CONCLUSIONS: Oral finasteride promotes scalp hair growth and prevents
further hair
loss in a significant proportion of men with male pattern hair loss.
With its generally good
tolerability profile, finasteride is a new approach to the management
of this condition, for
which treatment options are few. Its role relative to topical minoxidil
has yet to be
determined.
=============================================================
21.) Finasteride in the treatment of men with androgenetic alopecia.
Finasteride Male
Pattern Hair Loss Study Group.
=============================================================
J Am Acad Dermatol 1998 Oct;39(4 Pt 1):578-89
Kaufman KD, Olsen EA, Whiting D, Savin R, DeVillez R, Bergfeld W, Price
VH, Van
Neste D, Roberts JL, Hordinsky M, Shapiro J, Binkowitz B, Gormley GJ
Department of Clinical Research, Merck Research Laboratories, Rahway,
NJ 07065,
USA.
BACKGROUND: Androgenetic alopecia (male pattern hair loss) is caused
by
androgen-dependent miniaturization of scalp hair follicles, with scalp
dihydrotestosterone
(DHT) implicated as a contributing cause. Finasteride, an inhibitor
of type II
5alpha-reductase, decreases serum and scalp DHT by inhibiting conversion
of
testosterone to DHT. OBJECTIVE: Our purpose was to determine whether
finasteride
treatment leads to clinical improvement in men with male pattern hair
loss. METHODS: In
two 1-year trials, 1553 men (18 to 41 years of age) with male pattern
hair loss received
oral finasteride 1 mg/d or placebo, and 1215 men continued in blinded
extension studies
for a second year. Efficacy was evaluated by scalp hair counts, patient
and investigator
assessments, and review of photographs by an expert panel. RESULTS:
Finasteride
treatment improved scalp hair by all evaluation techniques at 1 and
2 years (P < .001 vs
placebo, all comparisons). Clinically significant increases in hair
count (baseline = 876
hairs), measured in a 1-inch diameter circular area (5.1 cm2) of balding
vertex scalp,
were observed with finasteride treatment (107 and 138 hairs vs placebo
at 1 and 2 years,
respectively; P < .001). Treatment with placebo resulted in progressive
hair loss. Patients'
self-assessment demonstrated that finasteride treatment slowed hair
loss, increased hair
growth, and improved appearance of hair. These improvements were corroborated
by
investigator assessments and assessments of photographs. Adverse effects
were minimal.
CONCLUSION: In men with male pattern hair loss, finasteride 1 mg/d
slowed the
progression of hair loss and increased hair growth in clinical trials
over 2 years.
=============================================================
22.) Genetic analysis of male pattern baldness and the 5alpha-reductase
genes.
=============================================================
J Invest Dermatol 1998 Jun;110(6):849-53 Related Articles, Books, LinkOut
Ellis JA, Stebbing M, Harrap SB
Department of Physiology, The University of Melbourne, Parkville, Victoria,
Australia.
Genetic predisposition and androgen dependence are important characteristics
of the
common patterned loss of scalp hair known as male pattern baldness.
The involvement of
the 5alpha-reductase enzyme in male pattern baldness has been postulated
due to its role
in the metabolism of testosterone to dihydrotestosterone. There are
two known isozymes
of 5alpha-reductase. Type I has been predominantly localized to the
skin and scalp. Type
II, also present on the scalp, is the target of finasteride, a promising
treatment for male
pattern baldness. We conducted genetic association studies of the 5alpha-reductase
enzyme genes (SRD5A1 on chromosome 5 and SRD5A2 on chromosome 2) using
dimorphic intragenic restriction fragment length polymorphisms. >From
a population
survey of 828 healthy families comprising 3000 individuals, we identified
58 young bald
men (aged 18-30 y) and 114 older nonbald men (aged 50-70 y) for a case
control
comparison. No significant differences were found between cases and
controls in allele,
genotype, or haplotype frequencies for restriction fragment length
polymorphisms of either
gene. These findings suggest that the genes encoding the two 5alpha-reductase
isoenzymes are not associated with male pattern baldness. Finally,
no clear inheritance
pattern of male pattern baldness was observed. The relatively strong
concordance for
baldness between fathers and sons in this study was not consistent
with a simple
Mendelian autosomal dominant inheritance. A polygenic etiology should
be considered.
=============================================================
23.) Effect of finasteride on human testicular steroidogenesis.
=============================================================
J Androl 1996 Sep-Oct;17(5):516-21 Related Articles, Books
Castro-Magana M, Angulo M, Fuentes B, Canas A, Sarrantonio M, Arguello
R, Vitollo
P
Department of Pediatrics, Winthrop-University Hospital, Mineola, New
York 11501,
USA.
We studied the testicular function and some androgen-mediated events
in 22 males
(16-30 years of age) with male pattern baldness that was treated with
finasteride (10 mg
once daily) for 2 years. Patients were evaluated every 3 months. Prostatic
volume was
determined in six subjects by endorectal ultrasound scans. Serum gonadotropin,
prostate-specific antigen (PSA), and sex hormone levels were determined
basally and
periodically during the treatment period. Fourteen subjects underwent
gonadal stimulation
with human chorionic gonadotropin (hCG), and the gonadotropin response
to
gonadotropin releasing hormone (GnRH) was determined in eight subjects,
prior to and
after 2 years of therapy. Finasteride treatment resulted in an improvement
in the male
pattern baldness and prostatic shrinkage that was associated with an
increase in serum
testosterone levels (17.2 +/- 2.5 vs. 26.3 +/- 1.7 nmol/L) and a decrease
in
dihydrotestosterone (DHT) levels (1.45 +/- 0.41 vs. 0.38 +/- 0.10 nmol/L),
causing a
marked increase in that testosterone/DHT ratio. A significant increase
in the serum levels
of androstenedione (3.67 +/- 0.49 vs. 7.05 +/- 0.70 nmol/L) and estradiol
(132 +/- 44
vs. 187 +/- 26 pmol/L) was also noted, whereas androstanediol glucoronide
(33.3 +/-
6.4 vs. 10.7 +/- 4.5 pmol) and PSA (1.6 +/- 0.6 vs. 0.4 +/- 0.1 ng/ml)
were significantly
decreased. No changes in basal or stimulated levels of gonadotropin
were observed.
There was a significant increase in the testosterone response to hCG
during finasteride
therapy (delta: 16.7 vs. 35.5 nmol/L) that could be explained, at least
in part, by the
reduction of testosterone metabolism resulting from the blockage induced
by finasteride.
The decrease in the androstenedione to testosterone and estrone to
estradiol ratios
observed after hCG treatment, however, strongly suggests increased
activity of the
17-ketosteroid reductase enzyme and an improvement of the testicular
capacity for
testosterone production.
=============================================================
24.) [Finasteride: a new drug for the treatment of male hirsutism and
androgenetic
alopecia]?
=============================================================
Clin Ter 1996 Jun;147(6):305-15 Related Articles, Books, LinkOut
[Article in Italian]
Spinucci G, Pasquali R
Dipartimento di Medicina interna e Gastroenterologia, Policlinico S.
Orsola-Malpighi,
Bologna.
Finasteride is a drug which inhibits the transformation of testosterone
into its active
metabolite, dihydrotestosterone, in the target organs, i.e. the skin,
the scalp, the liver and
the prostate. In the pathogenic mechanism of hirsutism and androgenetic
alopecia, and
important role is presumably played by alterations of the mechanisms
which transform
testosterone into dihydrotestosterone. In some conditions an increase
in
dihydrotestosterone has been demonstrated, due to increased activity
of the enzyme 5
alpha-reductase. The effect of finasteride develops above all at the
level of type II 5
alpha-reductase. Recent studies have evaluated the effect of finasteride
in patients of both
sexes with hirsutism and androgenetic alopecia. In women with various
forms of
hyperandrogenism, the use of the drug at the doses commonly used for
the treatment of
benign prostatic hyperplasia seems to have induced a significant reduction
in the degree of
hirsutism. Furthermore, both in animals and men with alopecia, the
drug seems to have led
to an increase in the number and an improvement in the shape of the
follicles in the anagen
phase, and a simultaneous decrease of dehydrotestosterone at the level
of the scalp. This
study represents a review of the main results obtained over the last
two years and reports
the prospects which the use of finasteride may have in this context.
=============================================================
25.) The 5 alpha-reductase system and its inhibitors. Recent development
and its
perspective in treating androgen-dependent skin disorders.
=============================================================
Dermatology 1996;193(3):177-84 Related Articles, Books, LinkOut
Chen W, Zouboulis CC, Orfanos CE
Department of Dermatology, University Medical Center Benjamin Franklin,
Free
University of Berlin, Germany.
5 alpha-Reductase, the enzyme system that metabolizes testosterone into
dihydrotestosterone, occurs in two isoforms. The type 1 isozyme is
composed of 259
amino acids, has an optimal pH of 6-9 and represents the 'cutaneous
type'; it is located
mainly in sebocytes but also in epidermal and follicular keratinocytes,
dermal papilla cells
and sweat glands as well as in fibroblasts from genital and non-genital
skin. The type 2
isozyme is composed of 254 amino acids, has an optimal pH of about
5.5 and is located
mainly in the epididymis, seminal vesicles, prostate and fetal genital
skin as well as in the
inner root sheath of the hair follicle and in fibroblasts from normal
adult genital skin. The
genes encoding type 1 and type 2 isozymes are found in chromosomes
5p and 2p,
respectively, and each consists of 5 exons and 4 introns. During the
last decade, several
steroid analogues and non-steroid agents have been developed to interfere
with 5
alpha-reductase activity. Finasteride, which has a higher affinity
for the type 2 isozyme, is
the first 5 alpha-reductase antagonist clinically introduced for treatment
of benign prostate
hyperplasia. The clinical evaluation of finasteride or other 5 alpha-reductase
inhibitors in
the field of dermatology has been very limited; in particular, those
that selectively bind to
type 1 isozyme (e.g. MK-386, LY191704) may be regarded as candidates
for treatment
of androgen-dependent skin disorders such as seborrhoea, acne, hirsutism
and/or
androgenetic alopecia.
=============================================================
26.) Finasteride: a clinical review.
=============================================================
Biomed Pharmacother 1995;49(7-8):319-24 Related Articles, Books
Gormley GJ
Merck Research Laboratories, Rahway, NJ 07065-0914, USA.
Finasteride is the first of a new class of 5 alpha-reductase inhibitors
which allows selective
androgen deprivation affecting dihydrotestosterone (DHT) levels in
target organs such as
the prostate and scalp hair without effecting circulating levels of
testosterone thus
preserving the desired androgen mediated effects on muscle strength,
bone density and
sexual function. Finasteride has been demonstrated to produce significant
effects in men
with an enlarged prostate gland. The long-term data now emerging suggests
that
progression of benign prostatic hyperplasia (BPH) may be arrested providing
additional
long term benefits. Experimental uses in prostate cancer prevention
and male pattern
baldness offer new and exciting possibilities for this class of compounds.
=============================================================
27.) The effect of finasteride, a 5 alpha-reductase inhibitor, on scalp
skin testosterone and
dihydrotestosterone concentrations in patients with male pattern baldness.
=============================================================
J Clin Endocrinol Metab 1994 Sep;79(3):703-6 Related Articles, Books,
LinkOut
Dallob AL, Sadick NS, Unger W, Lipert S, Geissler LA, Gregoire SL, Nguyen
HH,
Moore EC, Tanaka WK
Merck Research Laboratories, Rahway, New Jersey 07065.
The effects of the 5 alpha-reductase inhibitor, finasteride, on scalp
skin testosterone (T)
and dihydrotestosterone (DHT) levels were studied in patients with
male pattern baldness.
In a double blind study, male patients undergoing hair transplantation
were treated with
oral finasteride (5 mg/day) or placebo for 28 days. Scalp skin biopsies
were obtained
before and after treatment for measurement of T and DHT by high pressure
liquid
chromatography-RIA. In 10 male subjects studied at baseline, mean (+/-
SEM) DHT
levels were significantly higher in bald (7.37 +/- 1.24 pmol/g) compared
to hair-containing
(4.20 +/- 0.65 pmol/g) scalp, whereas there was no difference in mean
T levels at
baseline. In bald scalp from 8 patients treated with finasteride, the
mean DHT
concentration decreased from 6.40 +/- 1.07 pmol/g at baseline to 3.62
+/- 0.38 pmol/g
on day 28. Scalp T levels increased in 6 of 8 subjects treated with
finasteride. Finasteride
decreased the mean serum DHT concentration from 1.36 +/- 0.18 nmol/L
(n = 8) at
baseline to 0.46 +/- 0.10 nmol/L on day 28 and had no effect on serum
T. There were no
significant changes in scalp or serum T or DHT in placebo-treated patients.
In this study,
male subjects treated with 5 mg/day finasteride for 4 weeks had significantly
decreased
concentrations of DHT in bald scalp, resulting in a mean level similar
to the baseline levels
found in hair-containing scalp.
=============================================================
28.) Finasteride: the first 5 alpha-reductase inhibitor.
=============================================================
Pharmacotherapy 1993 Jul-Aug;13(4):309-25; discussion 325-9 Related
Articles,
Books
Sudduth SL, Koronkowski MJ
Program on Aging, School of Pharmacy, University of North Carolina,
Chapel Hill
27599-7360.
Finasteride is a synthetic 4-azasteroid that is a specific competitive
inhibitor of 5
alpha-reductase, an intracellular enzyme that converts testosterone
to dihydrotestosterone
(DHT). It has no binding affinity for androgen receptor sites and itself
possesses no
androgenic, antiandrogenic, or other steroid hormone-related properties.
It is well
absorbed after oral administration, with absolute bioavailability in
humans of 63% (range
34-108%). The mean time to maximum concentration is 1-2 hours, and
it is
approximately 90% plasma protein bound. The elimination half-life averages
6-8 hours.
The agent is metabolized to a series of five metabolites, of which
two are active and
possess less than 20% of the 5 alpha-reductase activity of finasteride.
Little is known
about potential drug interactions, although they appear to be minimal
and not clinically
relevant. The drug is indicated for the treatment of symptomatic benign
prostatic
hyperplasia. Its efficacy in regression of prostate gland enlargement
is rapid and
predictable, although correlation with subsequent improvement in urinary
flow and
symptoms is highly variable. Dosages of 0.5-100 mg/day regress prostate
enlargement;
the recommended dosage is 5 mg once/day. Finasteride may hold promise
for other
DHT-mediated disorders such as acne, facial hirsutism, frontal lobe
alopecia, and
prostate cancer, but its use in these conditions remains investigational.
The frequency of
adverse drug events is low, with the most common side effects being
impotence,
decreased libido, and decreased volume of ejaculate. No reports of
intentional overdose
have been reported, and dosages of up to 80 mg/day for 3 months have
been taken
without adverse effect.
=============================================================
29.) Cytologic atypia in a 53-year-old man with finasteride-induced
gynecomastia.
=============================================================
Arch Pathol Lab Med 2000 Apr;124(4):625-7 Related Articles, Books,
LinkOut
Zimmerman RL, Fogt F, Cronin D, Lynch R
Departments of Pathology & Laboratory Medicine, Presbyterian Medical
Center,
University of Pennsylvania Health System, Philadelphia, PA 19104, USA.
Finasteride has been associated with the development of gynecomastia.
Although
cytoplasmic vacuolization has been noted in prostatic epithelium in
men taking this drug,
we found no documentation of the cytologic changes in finasteride-associated
gynecomastia. We present the case of a 53-year-old man who developed
unilateral
gynecomastia following finasteride therapy for alopecia. A fine-needle
aspiration biopsy of
the mass was diagnosed as adenocarcinoma on the basis of nuclear atypia
and particularly
because of cytoplasmic vacuolization. Subsequent excisional biopsy
revealed benign
gynecomastia with no evidence of malignant change. The ductal epithelium
did exhibit
cytoplasmic vacuolization similar to that described in the prostate
following finasteride
therapy. We believe this is the first reported case documenting the
cytologic changes seen
in gynecomastia secondary to finasteride therapy. Cytoplasmic vacuolization
in this setting
should not be considered evidence of malignancy in men with gynecomastia.
As with
gynecomastia in general, extreme caution should be used before rendering
a cytologic
diagnosis of malignancy.
=============================================================
30.) Reversible painful gynaecomastia induced by low dose finasteride
(1 mg/day).
=============================================================
Australas J Dermatol 2000 Feb;41(1):55 Related Articles, Books, LinkOut
Wade MS, Sinclair RD
Publication Types:
Letter
=============================================================
=============================================================
31.) Measuring reversal of hair miniaturization in androgenetic alopecia
by follicular counts
in horizontal sections of serial scalp biopsies: results of finasteride
1 mg treatment of men
and postmenopausal women.
=============================================================
J Investig Dermatol Symp Proc 1999 Dec;4(3):282-4 Related Articles,
Books, LinkOut
Whiting DA, Waldstreicher J, Sanchez M, Kaufman KD
Baylor Hair Research and Treatment Center, Baylor University Medical
Center, Dallas,
Texas 75246, USA.
Hair regrowth was evaluated by histologic analysis in men and women
treated for
androgenetic alopecia, by counting follicles in horizontal sections
of scalp biopsies. Serial
4mm punch biopsies were taken at baseline and after 12mo of treatment
from the
transitional area of hair thinning between normal hair and vertex balding
in men, and in an
area of frontal/parietal thinning in women. Horizontal sections of
reticular and papillary
dermis were read by one observer, blinded to patient, treatment, and
time. All terminal
hair bulbs, terminal anagen and telogen hairs, and vellus and vellus-like
miniaturized hairs
were counted. Twenty-six men aged 18-41y, comprising 14 on finasteride
1 mg daily and
12 on placebo, and 94 postmenopausal women, aged 41-60y, comprising
44 on
finasteride 1 mg daily and 50 on placebo, were evaluated. In the male
study, the terminal
hairs increased from a mean baseline count of 15.5-20.9 after 12mo
of finasteride, versus
17.3-18.3 in the placebo patients. The miniaturized hairs decreased
from 26.7 to 23.6
with finasteride versus 21.3-20.3 with placebo. The terminal-to-vellus
ratio increased
more in the finasteride than in the placebo patients, suggesting some
reversal of the
miniaturization process with finasteride. In the female study, no significant
differences in
follicular counts were found between the finasteride and placebo groups
after 12mo of
treatment. Follicular counts in horizontal sections provide an informative
adjunct to
noninvasive measures used in hair growth studies. Finasteride appears
to be capable of
reversing hair miniaturization in androgenetic alopecia in young to
middle-aged men, but
not in postmenopausal women.
=============================================================
32.) Improvement in androgenetic alopecia in 53-76-year-old men using
oral finasteride.
=============================================================
Int J Dermatol 1999 Dec;38(12):928-30 Related Articles, Books, LinkOut
Brenner S, Matz H
Department of Dermatology, Tel Aviv Sourasky Medical Center, Tel Aviv,
Israel.
Twenty-eight men with AGA, aged 53-76 years (mean, 65 years), were selected
to
participate in this trial from a double blind, placebo controlled,
multicenter study of
subjects with moderate symptoms of BPH. Patients received either finasteride
5 mg or
placebo daily for 24 months. Hair counts were performed at entry to
the study and at 6,
12, 18, and 24 months. Hair counts were made directly on the scalp
in a circular target
area 1 in in diameter, located in the center of a template. The template
was applied in
such a way that its counting window fell on the most balding scalp
area, which remained
the same for each patient.11 At each hair counting session, patients
were asked about
side-effects and questioned about their sex life. Time trend and differences
between
groups were examined using a one-way (treatment) MANOVA with repeated
measures
(baseline, 6, 12, 18, and 24 months). Additional two-tailed t-tests
were performed to
compare the two groups at each point of time. P < 0.05 was considered
to be significant.
=============================================================
33.) New topical antiandrogenic formulations can stimulate hair growth
in human bald
scalp grafted onto mice.
=============================================================
Int J Pharm 2000 Jan 20;194(1):125-34 Related Articles, Books, LinkOut
Sintov A, Serafimovich S, Gilhar A
Ben-Gurion University of the Negev, The Institutes for Applied Research,
PO Box 653,
Beer-Sheva, Israel. [email protected]
The purpose of this study was to test the ability of topical formulations
of finasteride and
flutamide to re-enlarge hair follicles in male-pattern baldness. This
was evaluated by an
experimental model of human scalp skin graft transplanted onto SCID
mice. A
comparison was made between formulations containing finasteride and
flutamide, and a
vehicle formulation in terms of the mean hairs per graft, length, diameter
of the shafts, and
structures of the growth stages of the hair. Flutamide and finasteride
had a significantly
higher effect (P<0.05) than the placebo in all the tested parameters,
but flutamide
demonstrated more hair per graft and longer hair shafts than finasteride
(P<0.05). The
number of hairs per graft for flutamide and finasteride groups were
1.22+/-0. 47 and
0.88+/-0.95 hairs/0.5 mm2 graft, respectively, versus 0. 35+/-0.6 hairs/graft
for
vehicle-treated graft. Similarly, hair lengths for flutamide and finasteride
were 5.82+/-0.50
and 4.50+/-0. 32 mm, respectively, versus 2.83+/-0.18 mm for the vehicle-treated
grafts.
An in vitro diffusion study of flutamide gel using hairless mouse skin
demonstrated the
beneficial effect of the vehicle composition in comparison with a hydroalcoholic
solution
or a gel containing no penetration enhancer. It is therefore suggested
that this topical
composition containing flutamide or finasteride may effectively result
in regression of
male-pattern baldness.
=============================================================
34.) Current management of androgenetic alopecia in men.
=============================================================
Eur J Dermatol 1999 Dec;9(8):606-9 Related Articles, Books, LinkOut
Wolff H, Kunte C
Klinik fur Dermatologie und Allergologie, Ludwig-Maximilians-Universitat,
Frauenlobstrasse 9-11, D-80337, Munchen, Germany. [email protected]
Androgenetic alopecia (AGA) is a common dermatological condition affecting
both men
and women. Until recently there has been little interest in AGA as
a clinical condition,
largely due to the lack of any genuinely effective treatment for it.
A number of "remedies"
exist, such as vitamin supplements, which are not generally harmful
but which have no
proven efficacy in promoting hair growth or preventing further hair
loss. Hair systems and
surgery provide camouflage for the symptoms but do not effect a cure.
By far the most
promising approaches to the treatment of AGA are drug therapies, such
as minoxidil and
finasteride. Finasteride, an inhibitor of the type II 5alpha-reductase
that converts
testosterone to dihydrotestosterone, has been shown to prevent further
hair loss, and
promotes new hair growth in the majority of the men taking part in
clinical trials. Tailored
drug approaches like this offer the greatest hope for the successful
future treatment of
alopecia.
=============================================================
35.) Immunohistochemical localization of types 1 and 2 5alpha-reductase
in human scalp.
=============================================================
Br J Dermatol 1999 Sep;141(3):481-91 Related Articles, Books, LinkOut
Bayne EK, Flanagan J, Einstein M, Ayala J, Chang B, Azzolina B, Whiting
DA, Mumford
RA, Thiboutot D, Singer II, Harris G
Merck Research Laboratories, PO Box 2000, Rahway, NJ 07065, USA.
[email protected]
The predominant form of 5alpha-reductase (5aR) in human scalp is 5aR1.
None the less,
clinical studies have shown that finasteride, a selective inhibitor
of 5aR2, decreases scalp
dihydrotestosterone and promotes hair growth in men with androgenetic
alopecia.
Immunolocalization studies were thus carried out to examine 5aR isozyme
distribution
within scalp and, in particular, to determine whether 5aR2 might be
associated with hair
follicles. 5aR2 was localized using both a rabbit polyclonal and a
mouse monoclonal
antibody. 5aR1 was detected with a mouse monoclonal antibody. The specificity
of these
reagents was demonstrated both by immunofluorescence and Western blot
analyses of
COS cells overexpressing human 5aR1 or 5aR2. When cryosections of scalp
from men
with androgenetic alopecia were stained with antibody against 5aR2,
using
immunoperoxidase avidin-biotin complex methodology, immunostaining
was observed in
the inner layer of the outer root sheath and, in more proximal regions
of the follicle, in the
inner root sheath. Staining was also prominent in the infundibular
region of the follicle, with
less intense staining extending throughout the granular layer of the
epidermis. Some
staining was also seen in sebaceous ducts. Similar results were obtained
with both the
polyclonal and monoclonal 5aR2 antibodies. In contrast, in scalp cryosections
stained
with antibody to 5aR1, no immunostaining was observed within hair follicles.
Intense
staining for the type 1 isozyme was, however, detected within sebaceous
glands. Our
immunolocalization data suggest that the results seen in clinical trials
of men with male
pattern hair loss treated with finasteride may be due, at least in
part, to local inhibition of
5aR2 within the hair follicle.
=============================================================
36.) The psychosocial consequences of androgenetic alopecia: a review
of the research
literature.
=============================================================
Br J Dermatol 1999 Sep;141(3):398-405 Related Articles, Books, LinkOut
Cash TF
Department of Psychology, Old Dominion University, Norfolk, VA 23529-0267,
USA.
Androgenetic alopecia is a common dermatological condition, with potentially
adverse
psychosocial sequelae. The present review critically examines scientific
evidence
concerning the effects of androgenetic hair loss on social processes
and psychological
functioning, as well as the psychosocial outcomes of medical treatments.
Research
confirms a negative but modest effect of visible hair loss on social
perceptions. More
importantly, androgenetic alopecia is typically experienced as a moderately
stressful
condition that diminishes body image satisfaction. Deleterious effects
on self-esteem and
certain facets of psychological adjustment are more apparent among
women than men
and among treatment-seeking patients. Various 'risk factors' vis-a-vis
the psychological
adversity of androgenetic alopecia are identified. Medical treatments,
i.e. minoxidil and
finasteride, appear to have some psychological efficacy. A conceptual
model is delineated
to explain the psychological effects of hair loss and its treatment.
Directions for needed
research are discussed. Strategies are presented for the clinical management
of
psychological issues among these patients.
=============================================================
37.) Clinical dose ranging studies with finasteride, a type 2 5alpha-reductase
inhibitor, in
men with male pattern hair loss.
=============================================================
J Am Acad Dermatol 1999 Oct;41(4):555-63 Related Articles, Books, LinkOut
Roberts JL, Fiedler V, Imperato-McGinley J, Whiting D, Olsen E, Shupack
J, Stough D,
DeVillez R, Rietschel R, Savin R, Bergfeld W, Swinehart J, Funicella
T, Hordinsky M,
Lowe N, Katz I, Lucky A, Drake L, Price VH, Weiss D, Whitmore E, Millikan
L, Muller
S, Gencheff C, et al
Northwest Cutaneous Research Specialists, Portland, Oregan, USA.
BACKGROUND: Androgenetic alopecia is a common condition of adult men.
Finasteride, a type 2 5alpha-reductase inhibitor, decreases the formation
of
dihydrotestosterone from testosterone. OBJECTIVE: Two separate clinical
studies were
conducted to establish the optimal dose of finasteride in men with
this condition.
METHODS: Men from 18 to 36 years of age with moderate vertex male pattern
hair loss
received finasteride 5, 1, 0.2, or 0.01 mg/day or placebo based on
random assignment.
Efficacy was determined by scalp hair counts, patient self-assessment,
investigator
assessment, and assessment of clinical photographs. Safety was assessed
by clinical and
laboratory measurements and by analysis of adverse experiences. RESULTS:
Efficacy
was demonstrated for all end points for finasteride at doses of 0.2
mg/day or higher, with
1 and 5 mg demonstrating similar efficacy that was superior to lower
doses. Efficacy of
the 0.01 mg dose was similar to placebo. No significant safety issues
were identified in the
trials. CONCLUSION: Finasteride 1 mg/day is the optimal dose for the
treatment of men
with male pattern hair loss and was subsequently identified for further
clinical
development.
=============================================================
38.) The effects of finasteride on scalp skin and serum androgen levels
in men with
androgenetic alopecia.
=============================================================
J Am Acad Dermatol 1999 Oct;41(4):550-4 Related Articles, Books, LinkOut
Drake L, Hordinsky M, Fiedler V, Swinehart J, Unger WP, Cotterill PC,
Thiboutot DM,
Lowe N, Jacobson C, Whiting D, Stieglitz S, Kraus SJ, Griffin EI, Weiss
D, Carrington
P, Gencheff C, Cole GW, Pariser DM, Epstein ES, Tanaka W, Dallob A,
Vandormael
K, Geissler L, Waldstreicher J
University of Oklahoma Health Sciences, Oklahoma City, USA.
BACKGROUND: Data suggest that androgenetic alopecia is a process dependent
on
dihydrotestosterone (DHT) and type 2 5alpha-reductase. Finasteride
is a type 2
5alpha-reductase inhibitor that has been shown to slow further hair
loss and improve hair
growth in men with androgenetic alopecia. OBJECTIVE: We attempted to
determine the
effect of finasteride on scalp skin and serum androgens. METHODS: Men
with
androgenetic alopecia (N = 249) underwent scalp biopsies before and
after receiving
0.01, 0.05, 0.2, 1, or 5 mg daily of finasteride or placebo for 42
days. RESULTS: Scalp
skin DHT levels declined significantly by 13.0% with placebo and by
14.9%, 61.6%, 56.
5%, 64.1%, and 69.4% with 0.01, 0.05, 0.2, 1, and 5 mg doses of finasteride,
respectively. Serum DHT levels declined significantly (P <.001)
by 49.5%, 68.6%,
71.4%, and 72.2% in the 0.05, 0.2, 1, and 5 mg finasteride treatment
groups,
respectively. CONCLUSION: In this study, doses of finasteride as low
as 0.2 mg per
day maximally decreased both scalp skin and serum DHT levels. These
data support the
rationale used to conduct clinical trials in men with male pattern
hair loss at doses of
finasteride between 0.2 and 5 mg.
=================================================================
DERMAGIC/EXPRESS 2-(95) 25 Septiembre 2.000 25 September 2.000
Dr. JOSE LAPENTA R
==================================================================
|