ANOREXIA NERVOSA:

WHAT IS IT?
Anorexia nervosa, a psychophysiological eating disorder that typically develops in otherwise healthy individuals, literally translates to "no appetite, caused by nervousness." It should be distinguished from the word "anorexia" as used elsewhere in medicine to indicate loss of appetite in connection with a medical problem � for example, the diminished appetite that occurs in cancer or depression.
Anorexia nervosa is actually defined not so much by appetite as by weight loss. Most people with this disorder do feel hunger, but they disregard it, dieting to the point of starvation. The German term is somewhat more accurate: Pubert�tsmagersucht, or pubertal yearning for thinness.


Described in the medical litterature as far back as the 17th century, in modern times anorexia nervosa is most common in industrialized societies where thinness is equated with attractiveness. The problem usually begins in adolescence, often as secondary sexual characteristics are developing. The vast majority of those affected (about 90 percent) are girls or women, amounting to about three-quarters of a percent of all females in the United States. Food restriction can occur with varying degrees of intensity, but the problem is considered a disorder when the person weighs 15 percent less than her ideal body weight.
The person who develops this disorder fears being fat, and may have a deep but faulty conviction that she is overweight despite what the scale says. To achieve or maintain leanness, she may exercise obsessively or use laxatives. Since a super-restrictive diet requires exquisite control, she may become quite careful, inhibited and controlled in other spheres of life (for example, retreating from social contacts or adopting behavior rituals).
HOW COMMON IS ANOREXIA:
Studies show that 1% of women suffer from anorexia,in the 12-25 years old range.As for bulimia, it would be 3 times higher.However,those numbers do not incorporate young women refusing to admit they have a problem, even though their food intake is hardly ever higher then 300 calories a day..
Here is the diagnostic criterias,from the "Diagnostic and Statistical Manual of Mental Disorders" (DSM-IV):
Diagnostic criteria for 307.51 Anorexia Nervosa
|
A. Refusal to maintain body weight at or above a minimally normal weight for age and height (e.g., weight loss leading to maintenance of body weight less than 85% of that expected; or failure to make expected weight gain during period of growth, leading to body weight less than 85% of that expected).
|
B. Intense fear of gaining weight or becoming fat, even though underweight. |
|
C. Disturbance in the way in which one's body weight or shape is experienced, undue influence of body weight or shape on self-evaluation,or denial of the seriousness of the current low body weight. |
|
D. In postmenarcheal females,amenorrhea, i.e., the absence of at least three consecutive menstrual cycles. (A woman is considered to have amenorrhea if her periods occur only following hormone, e.g., estrogen, administration.) |
| *Specify type:
Restricting Type: during the current episode of Anorexia Nervosa,the person has not regularly engaged in binge-eating or purging behavior (i.e., self-induced vomiting or the misuse of laxatives,diuretics, or enemas)
Binge-Eating/Purging Type: during the current episode of Anorexia Nervosa,the person has regularly engaged in binge-eating or purging behavior (i.e., self-induced vomiting or the misuse of laxatives,diuretics, or enemas)
|
WHO IS AT RISK?
Anorexia is most likely to begin sometime between adolescence and the early 20s, but it can appear in children under the age of 10 or in women as old as 70. Although the disorder receives a great deal of publicity, it's relatively rare. For example, among teenage girls�the group at highest risk�the rate of anorexia is under 1 percent. While the disorder is most common among the middle and upper classes, it occurs in all social classes and ethnic groups.
Certain personality traits increase the risk of developing anorexia. Anorectic girls are often described as �model children� or perfectionists. Many have overcontrolling parents who are themselves fascinated by fitness and appearance. Faced with the impossible task of always being perfect, these girls discover that they can take charge of at least one aspect of their lives by exerting control over their eating and their weight.
Family background may also predispose a woman to anorexia.If you have a mother or sister with anorexia,you are7 to 12 times more likely to have the problem than if there were no history of the disorder in your family.However,in a number of cases, there is no familial link.
Perfectionnistic, over acheiving girls,with an excessive need to control themselves as well as their environment.They are often people pleasers,with an extreme need of approval from others.It's ever so easy to go,harder to find your wayback. Once trapped,the battle has begun. Being in a constant starving state,one suffering from anorexia experience a strong feeling of control and power over a body she hates so much...
Some clinicians believe that the symptoms of anorexia are a kind of symbolic language used by people who don't know how to, or are afraid to, express powerful emotions directly, with words. For example, making one's body tiny and thin may substitute for, "I'm not ready to grow up yet," or "I'm starving for attention." Refusing to eat may translate to "I won't let you control me!"
WHY IT HAPPENS?
Anorexia and eating disorders are unhealthy responses to stress,painful feelings,and other problems.While the specific cause is unknown,the condition seems to stem from a combination of psychological,biological,familial,and cultural factors.
The teens and early twenties are tumultuous years for a woman.Moods and emotions can swing wildly from one day to the next.The dutiful daughter turns into the rebel,eager to assert her independence�sometimes in self-destructive ways. Some researchers see anorexia as a power struggle between a strong�willed girl and her dominating parents.Starving herself,she unconsciously shows that she is in control of her own body and affirms that her parents are powerless to stop her.Since anorexia usually causes menstrual periods to stop and breasts to flatten,other experts theorize that girls who refuse to eat may be expressing a desire to remain children,free of adult bodies,adult sexual relationships,and adult responsibilities.
Stress can play a major role in anorexia.Taking an exam,moving to a new home,starting college or a new job,becoming pregnant,and beginning or ending a relationship may sometimes push a woman into beginning the heavy dieting that ends with anorexia.
Our equation of thinness with beauty, social success, and even desirability is also at fault. In America, the pressure to be thin is intense. Most young women can handle it successfully, but a few respond in extreme ways, such as anorexia. For some adolescents, ordinary biology poses a problem. As their bodies mature, many girls discover that they can no longer eat as they used to without gaining weight.Most can cut back as needed; a few lose control. Sensible dieting is fine,but when low calories become no calories,it's time to admit there's a problem.
-PREDISPOSING FACTORS:
Many children and young adults can cope with stressful life events without developing any mental health problems.Therefore,those who do may have a predisposing risk that increases their likelihood of developing an eating disorder.Personality characteristics such as perfectionism may increase a persons chances of developing an eating disorder, and more recent research suggests that there may be a genetic influence involved.
Predisposing environmental factors may include stress or adversities.There maybe background stressful life situations such as problems within family dynamics or dissatisfaction with family life.In addition,the sufferer may have inadequate coping skills or be unable to talk about their emotions or problems. This may lead them to bottle up anxieties and channel them through dieting as a coping mechanism.
People who develop anorexia often feel stressed and anxious when faced with new situations.Many are perfectionists who have low tolerance for change (including the normal physical changes their bodies experience at puberty),feeling that it represents chaos and loss of control.Some set rigid,unrealistic standards for themselves and feel they have failed totally when they cannot achieve and maintain the degree of excellence they demand of themselves.
PSYCHOLOGICAL MOTIVATION OF ANOREXIA:
Studies are showing that people with anorexia actually get a euphoric feeling when they are hungry and denying themselves food. As they continue to starve the brain releases hormones that give them a �high� feeling, similar to the �high� that runners get when running long distances. The thinner they are; the more control they exert over their hunger, the more successful they feel. Anorexics are unaware of their problem with food; they feel normal.
WHAT CAUSES IT?
The cause of anorexia nervosa is not clear. It is likely the consequence of both genetic and environmental factors. Some of the proposed causes include:
A variant of depression or anxiety � Anorexia, depression, anxiety and obsessive-compulsive disorder tend to run in families, and many individuals with anorexia nervosa have symptoms of depression or obsessive-compulsive disorder.
|
|
A consequence of fears about becoming an adult� One such fear, for example, may be fear of the sexual experimenting that begins in adolescence. In girls, if dieting progresses far enough, the onset of menstruation may be delayed or may stop once started, halting one element of sexual development. |
Environmental Pressures� Images from TV and film and pressure from peers leave the impression that thin is best. |
Difficult family relationships� Although these difficulties have been suggested as a cause of the illness, they may actually follow its onset, because a person with anorexia nervosa may test the patience of those she lives with. People with the disorder describe a feeling of power and control over others through their dieting. |
In advanced stages of the illness,the dieting is hard to reverse.Hunger may then disappear completely and the pursuit of thinness becomes a way of life.Starvation causes medical complications of its own,such as thyroid problems,anemia and joint pains.Death can occur in the most severe cases,most commonly because of an irregular heartbeat caused by an imbalance of the salts in the bloodstream.
PRECIPITATING FACTORS:
There may be a preceding event,which may trigger the onset of the condition.Anorexia nervosa is often preceded by a period of continuous dieting.Many sufferers begin to diet after an unkind comment,perhaps relating to their weight,or just as a teenage preoccupation,or because they see others dieting.
However,*triggers may be unrelated to weight or dieting*.The upheaval following life changes such as:
- moving;
- school;
- bereavement;
- divorce;
- other emotional trauma (involving loss of separation or which injure their sense of self-worth) may be sufficient to trigger an onset.
Events may occur to be threatened which they feel powerless to change or prevent,and may lead them to seek solace in an activity where they can exercise complete control and find a sense of security.
"But why dieting?"
The message we receive from the media about weight and body shape is that thinness epitomises success,beauty and self control.In this context the sufferer may view thinness as a practical and measurable way of achieving control or security in their life if they believe that it is otherwise lacking.
PERPETUATING FACTORS:
Anorexia Nervosa may appear to solve some of the sufferers immediate problems, and thus create a vicious circle,which traps them in the behaviours of the eating disorder.They may experience gratification at losing the weight,as it may make them feel in control,powerful,successful or safe.They may also feel rewarded by the increase of attention they receive due to concern from others about their weight.Their illness may become the centre of their families attention and therefore serves the function of distracting the family away from other problems they may have.
As the family comes together in concern for the sufferer,the eating disorder begins to replace the problems that may have previously threatened family stability.In this way,weight loss appears to serve a function and the sufferer will be reluctant to stop,or to even want to change.
There are other ways in which the disorder may become self-perpetuating.For example,as the sufferer becomes more preoccupied with food and avoids situations where they may have to eat with others,they become more socially isolated,which may further decrease their self-esteem.As mentioned previously, the sufferer may experience all-or-nothing thinking,which decreases their chance of loosening their dieting pattern.Any deviation from their tight restrictions will be percieved as utter failure.

Many of these factors interact with the physical consequences of weight loss,making established patterns more difficult to change.There are also other problems which may maintain the 'vicious circle',such as feeling happier after weight loss or vomiting,or a lack of control.An important factor in breaking such cycles is the quality and continuity of support the individual receives both in and out of treatment.
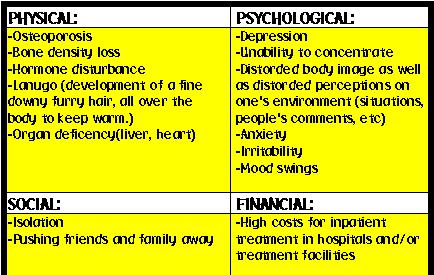
CONSEQUENCES OF ANOREXIA:
EXPECTED DURATION:
The course and therefore the duration of anorexia nervosa are very varied. Some people have a single relatively brief episode after experiencing an isolated stressful event. For others the problem becomes chronic and the condition gradually deteriorates. Many people start by restricting food, then later binge and purge. Although the majority of cases resolve by late adolescence, a significant number of people have persistent problems with diet and body image into adulthood.
HOSPITALIZATION CRITERIAS:
Severe weight loss and malnutrition:
-Weight <75% of ideal body weight;
-Weight loss of (>/=)=30% in 3 mo;
-BMI < 14 and inability/unwillingness to gain weight. |
| Dehydration |
Electrolyte abnormalities:
-Hypokalemia, especially if K is <2.5 mmol/L;
-Prolonged QTc;
-Arrhythmia;
-Marked hypophosphatemia (<1.0 mg/dL)
|
Physiologic instability:
-Severe bradycardia (<40 bpm);
-Hypotension (systolic BP <70);
-Hypothermia (<35�C);
-Orthostatic changes in HR and BP, syncope. |
| Arrested growth and development |
| Failure of outpatient treatment:=>(usually 3-6 mo,but sooner if medical condition deteriorates) |
| Acute food refusal |
| Uncontrollable binge eating and purging |
Acute medical complications of malnutrition:
-Syncope;
-Seizures (hypoglycemic,hyponatremic,bupropion and other medications)
-Cardiac failure;
-Arrhythmia;
-Mallory-Weiss esophageal tear;
-Gastric rupture;
-Pancreatitis
|
Acute psychiatric emergencies:
-Suicidal ideation;
-Acute psychosis
|
Comorbid diagnosis that interferes with treatment of the eating disorder:
-Severe depression
-Obsessive-compulsive disorder;
-Severe family dysfunction;
-Substance abuse |
CAN ANOREXIA BE PREVENTED?
There is no known preventive strategy.Early detection is key.Awareness on the part of parents and medical care providers,is needed.Early diagnosis and treatment can help prevent serious medical and psychological problems from developing and increase the chance of regaining good health.
So,if you think you may have anorexia nervosa,talk with your health care provider or a mental health professional.If you think someone you know may have anorexia nervosa,encourage her or him to get professional help.
TREATMENT OPTIONS:
Anorexia nervosa is best treated by a combination of psychotherapy and medication. If medical problems develop as a consequence of starvation, medical treatment may also be required. In a minority of cases, hospitalization may be called for, either to address the problematic behavior related to food or to treat medical complications.The first problem to address, especially when a person�s weight is dangerously low, is getting the weight in a safe range. This is a tremendous challenge since often the person with the illness does not openly discuss eating as a problem. Progress depends upon defining the problem in a way the person can accept, then working toward common goals.
Once the problem is acknowledged, a variety of therapy techniques can be helpful. A nutritionist can plan a healthy eating program that promotes slow weight gain. Cognitive behavior therapy encourages the recognition of flawed thoughts about body image, food and dieting, and helps to control the anxiety about eating. Family therapy may be important, both to provide support and education to family members and to examine interactions that may be unhelpful to every family member.
Later, when symptoms are under better control, the person with anorexia nervosa may want to understand the meaning of the symptoms, including how they may have affected important relationships, limited emotional growth and altered self-concept. It may also then be possible to look at what underlying problems may have led to the eating problem in the first place.
RECOVERY/PROGNOSIS:
WHAT IS THE OUTCOME WITH TREATMENT?
Although weight gain can occur quickly once treatment begins,complete recovery can take a number of years.Many of those who recover in terms of weight remain overly concerned about eating and weight.Relapse can occur during periods of stress.
About 75% of people with anorexia nervosa continue to show improvement after initial treatment.
- About 45% of these people have an excellent outcome;
- Another 30% experience considerable improvement;
- About 20% of those receiving treatment remain seriously impaired.
|
Between 2% and 10% die because of the disorder.Deaths are usually related to complications of starvation or suicide.However,death rates appear to be decreasing due to improved treatments.
Factors associated with successful recovery include:
-Motivation to change
-Young age when anorexia nervosa starts
-Short length of illness
-Absence of binge eating or purging
However, recovery is possible in those who have had anorexia nervosa for many years and who have not succeeded with previous treatments. With proper treatment and a strong desire to change, people with anorexia nervosa can go on to live healthy, productive, and satisfying lives.
Many people have milder forms of anorexia nervosa and are quite amenable to treatment, particularly when a variety of treatments are combined.For those who have lost a great deal of weight and are medically compromised, aggressive treatment can reverse a downward course.Unfortunately a significant percentage of those hospitalized for medical complications of anorexia nervosa are so resistant to treatment that they do not survive, but a majority do respond to treatment and have a full or nearly full recovery.
Although medications, particularly antidepressants, have been shown to be more effective treatment for bulimia than for anorexia nervosa, there is some evidence that antidepressant treatment is useful in anorexia. Medication may be most effective for those who have symptoms of depression, anxiety or obsessive-compulsive disorder. Selective serotonin reuptake inhibitors, such as fluoxetine(Prozac), sertraline (Zoloft) and paroxetine (Paxil), are frequently tried.
Distorted thinking about food may reach psychotic proportions, and in those cases treatment may include an antipsychotic medication. The newer drug olanzapine has a side effect that in this case is a benefit � it often causes weight gain.
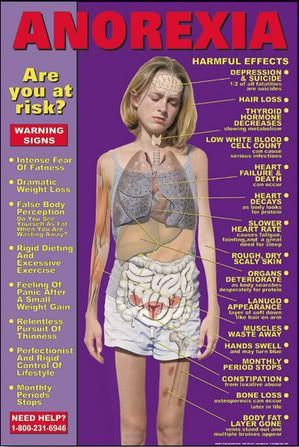
Go on SERIOUS complications of anorexia nervosa
You think you're alright? Mmm...Take a look at this poster and see for yourself:
INTERESTING THINGS TO CHECK OUT FOR MORE INFORMATION:
HOME
� copyright Cath's ED Website 2002-2003-2004