 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
 |
|
|
Rhinology/Allergy pages |
|
|
|
|
|
Sinus Surgery |
|
|
|
|
|
 |
|
|
|
|
|
|
Sinus surgery has advanced tremendously over what could be accomplished in the past. Our understanding of sinus disease has greatly benefitted from the introduction of CT scans and nasal fiberoptic endoscopes. These same endoscopes are also used in the operating room to allow a sinus surgeon to accurately operate upon the areas of disease. The surgery is much easier on the patients, and is more effective. Sinus surgery still has considerable risks though, as the surgeon is operating between the eyes and below the brain. You want your sinus surgeon to be very well versed in their field. Stereotactic localization systems are available to help surgeons open sinuses which have altered anatomy from prior surgery, etc.
Endoscopic sinus surgery typically takes 1 to 3 hours in the operating room. It can be done under sedation or general anesthesia (i.e., fully asleep). It is typically performed on an outpatient basis. The pain is mild or moderate � similar to being struck in the nose with a door. Packing is not usually required; packing is miserable for the patient, and most would prefer some mild bloody drainage over packing.
Patients usually take one week off from work, although some are able to go back sooner; this depends upon the extent of dissection necessary and the individual�s tolerance. The patient will follow up in the office after the surgery at 1, 2, and 4 weeks. Endoscopic cleaning of the defect is performed at these sessions.
80 to 90% of the patients who undergo endoscopic sinus surgery are pleased with their results. |
|
|
|
 |
|
|
|
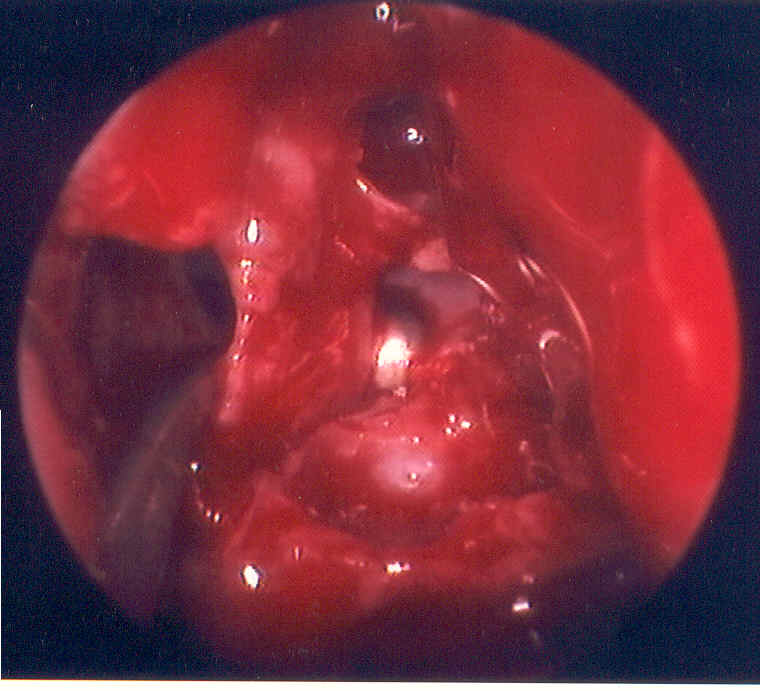
This picture was taken during a typical case. The patient presented with acute exacerbations of chronic rhinosinusitis. The picture illustrates an opening into a concha bullosa, or a sinus within the middle turbinate, on the patient's right side. The lateral wall of this sinus will be removed to provide drainage for this sinus, and improve the drainage pathways for the other surrounding sinuses. There is always some bleeding, but with good vasoconstriction it is not too voluminous. This patient went on to heal very nicely and felt "a hundred times better." |
|
|
|
 |
|
|
|
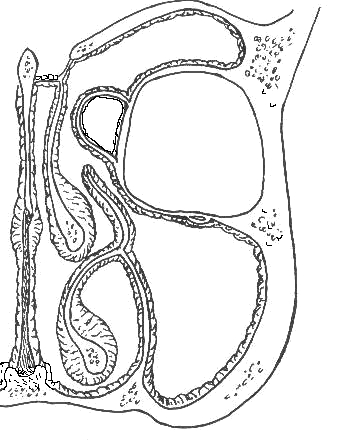
The picture above displays the outflow tract for the ethmoid bulla. Attention to details, such as removing the bridge of tissue around this tract, leads to more rapid healing and more successful surgery |
|
|
|
Return to start |
|