|
The Pituitary Gland
The pituitary gland
lies posterior/superior to the sphenoidal sinus
Development
Arterial supply
and venous drainage
Histology
Posterior pituitary
Clinical Anatomy
Form, position and relations

The pituitary gland lies in the hypophyseal fossa of the sphenoid and is
connected to the hypothalamus by the infundibulum, or pituitary stalk. The dura
covering the superior aspect of the gland forms the diaphragma sella. The gland
is about 12mm transversely and 8mm in anteroposterior diameter. The major
divisions of the gland are the anterior lobe, or adenohypophysis, and the
posterior lobe, the neurohypophysis. Each of these major subdivisions, which have different embryological origins, is further subdivided:
subdivisions, which have different embryological origins, is further subdivided:
- Adenohypophysis
- pars distalis
- pars intermedia
- pars tuberalis
- Neurohypophysis
- pars nervosa
- pituitary stalk
- median emminence
The pituitary gland lies posterior/superior to the sphenoidal sinus
The pituitary gland is derived from
 two
sources. The anterior lobe is an upgrowth of ectoderm from the roof of the
stodeum, while the posterior lobe is a down growth of neurectoderm from the
diencephalon. In the middle of the fourth week, a diverticulum, Rathke's
pouch, grows upwards from the roof of what will become the mouth
towards the developing brain. As the upgrowth contacts a down growth from the
brain, the infundibulum, it begins to pinch off from its
connection with the stomodeum. By the sixth week the connection between Rathke's
pouch and the oral cavity degenerates. The cells of Rathke's pouch proliferate
to form the pars distalis, and extend up the anterior aspect of the infundibulum
as the pars tuberallis. The posterior surface of Rathke's pouch does not
proliferate but forms the poorly developed pars intermedia. The infundibulum
having grown down from the floor of the diencephalon, expands as the axons of
cells in the diencephalon grow down into it. two
sources. The anterior lobe is an upgrowth of ectoderm from the roof of the
stodeum, while the posterior lobe is a down growth of neurectoderm from the
diencephalon. In the middle of the fourth week, a diverticulum, Rathke's
pouch, grows upwards from the roof of what will become the mouth
towards the developing brain. As the upgrowth contacts a down growth from the
brain, the infundibulum, it begins to pinch off from its
connection with the stomodeum. By the sixth week the connection between Rathke's
pouch and the oral cavity degenerates. The cells of Rathke's pouch proliferate
to form the pars distalis, and extend up the anterior aspect of the infundibulum
as the pars tuberallis. The posterior surface of Rathke's pouch does not
proliferate but forms the poorly developed pars intermedia. The infundibulum
having grown down from the floor of the diencephalon, expands as the axons of
cells in the diencephalon grow down into it.
The arteries of the pituitary gland arise from the internal carotid arteries
as the inferior and superior hypophyseal arteries. The inferior hypophyseal arteries mainly supply the pars nervosa before forming
short portal vessels to supply the pars distalis. The superior hypophyseal
arteries supply the floor of the hypothalamus, the median eminence. The
capillary plexus formed by the superior hypophyseal artery in the median
eminence form into long portal vessels which run down in the pituitary stalk to
form a capillary plexus in the pars distalis. In the median eminence the
capillary plexus receives secretions from releasing factor cells.
The inferior hypophyseal arteries mainly supply the pars nervosa before forming
short portal vessels to supply the pars distalis. The superior hypophyseal
arteries supply the floor of the hypothalamus, the median eminence. The
capillary plexus formed by the superior hypophyseal artery in the median
eminence form into long portal vessels which run down in the pituitary stalk to
form a capillary plexus in the pars distalis. In the median eminence the
capillary plexus receives secretions from releasing factor cells.
The blood is drained from the pituitary by inferior hypophyseal veins into
the dural venous sinuses.
Anterior pituitary
The anterior pituitary is formed of a range of cells producing several
hormones. An essential component in the organization and function of the anterior pituitary is the close relationship between the cells
and the capillary bed. The access to the circulation promotes uptake of the
substrate for hormone synthesis and allows efficient release of hormones into
the systemic circulation. The activity of the cells of the anterior pituitary is
controlled through the presence of releasing factors present in the capillary
blood. The releasing factors are formed by hypothalamic cells and released into
the hypophyseal portal circulation. There are five distinct types of endocrine
cell, distributed either throughout the pars distalis or localized to particular
parts.
function of the anterior pituitary is the close relationship between the cells
and the capillary bed. The access to the circulation promotes uptake of the
substrate for hormone synthesis and allows efficient release of hormones into
the systemic circulation. The activity of the cells of the anterior pituitary is
controlled through the presence of releasing factors present in the capillary
blood. The releasing factors are formed by hypothalamic cells and released into
the hypophyseal portal circulation. There are five distinct types of endocrine
cell, distributed either throughout the pars distalis or localized to particular
parts.
- Somatotrophs are found mainly in the lateral extensions of the lobe,
secreting growth hormone.
- Corticotrophs are found mainly in the centre of the lobe, secreting
adrenocoticotrophic hormone, beta-lipotrophin, alpha-melanocyte stimulating
hormone and beta-endorphin.
- Thyrotrophs are concentrated mainly in the anterior of the lobe, secreting
thyroid stimulating hormone.
- Lactotrophs, scattered throughout the lobe, secreting prolactin.
- Gonadotrophs, also scattered throughout the lobe, secreting follicle
stimulating hormone and luteinizing hormone.
These cells can be identified by various means. Early histological methods
were based on the affinity for acidic and basic dyes. This resulted in cells
being described as acidiphils, basophils or chromophobes which did not take up
dye. Modern methods of identification are based on immunohistochemical
identification of hormones and by the ultrastructural appearance of the cells.
Control of the hormone producing cells of the pars distalis is through
secretion by cells of the hypothalamus.
- Growth hormone releasing hormone (GHRH) is produced by cells of the
arcuate nuclei.
- Growth hormone inhibiting hormone (somatostatin) is produced by the
paraventricular nuclei.
- Corticotropin releasing hormone (CRH) is released from cells of the
anterior part of the paraventricular nuclei.
- Thyrotropin releasing hormone (TRH) is produced by cells of the
dorsomedial nuclei.
- Prolactin release inhibiting hormone (dopamine) controlling the
lactotrophs is produced by the cells of the arcuate nuclei.
- Gonadotropin releasing hormone (GnRH) is produced mainly by the cells of
the arcuate nuclei and preoptic area.
The pars intermedia is not well developed and it is thought that its cells
produce pre-pro-opiomelanocortic peptides. The pars tuberalis is formed mainly
of gonadotrophs.
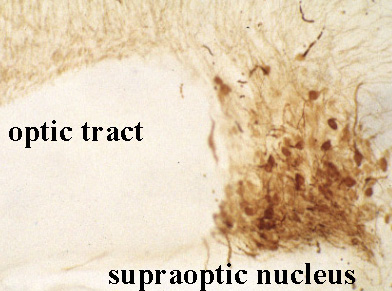
The posterior lobe or neurohypophysis is a continuation from the
hypothalamus. The hormone producing cells are located in the supraoptic and
paraventricular nuclei of the hypothalamus. The axons of these neurons run down
the pituitary stalk to terminate on the capillary bed of the posterior lobe. The
terminals are separated and grouped by glial cells, the pituicytes. The axons of
the hormone producing cells can be seen to contain numerous small clear
vesicles, and larger dense core vesicles.
Upward growth of pituitary tumours may press on the optic chiasma. Typical
visual field defects would be bitemporal hemianopia, and upper quadrantopia.
Tumours can grow up into the third ventricle causing hydrocephalus. Rapid lateral
expansion, perhaps due to haemorrhage may compress the third, fourth or sixth
cranial nerves. Headache may be present from stretch of the meninges. Surgery to
remove pituitary tumours is usually performed through the sphenoidal sinus.
This Page, its Graphics
and information are gratefully captured from the web of the
Faculty of Medicine
Memorial University of Newfoundland - Unfortunately these pages seem to have
expired.
 Australian
Pituitary Foundation. Australian
Pituitary Foundation.
é |